Download to read offline

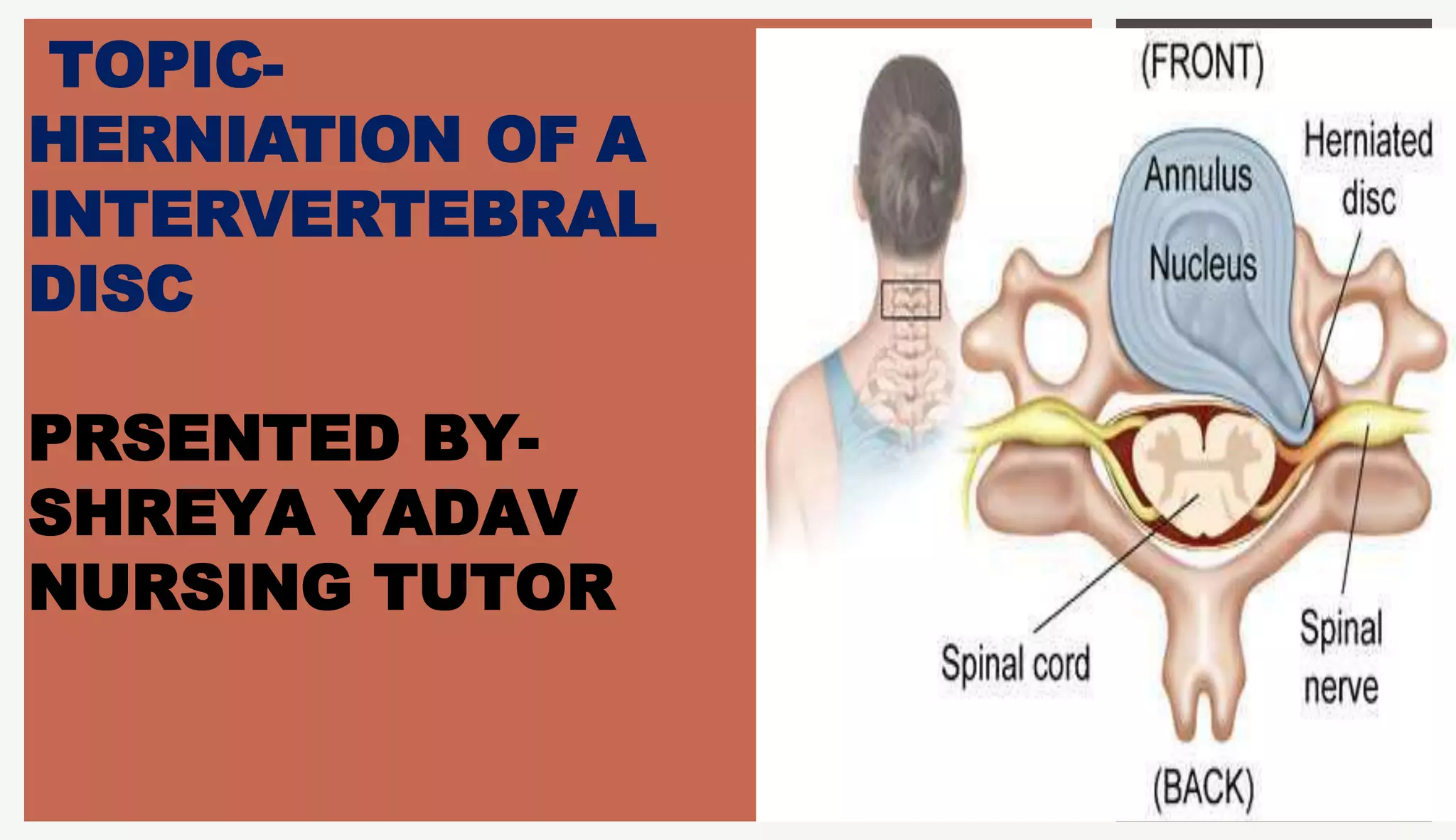

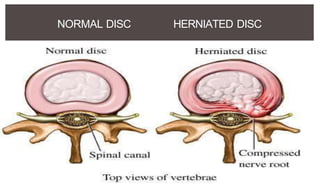




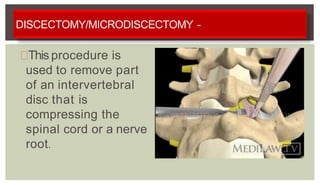

1. A herniated disc occurs when the soft central portion of an intervertebral disc bulges out beyond the damaged outer rings, most commonly in the lumbar region of the spine. 2. Symptoms vary depending on location but often include back pain radiating into the legs as well as sensory changes and weakness. 3. Treatment options include medications, physical therapy, epidural steroid injections, and surgery if conservative measures fail or neurological deficits are present.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


