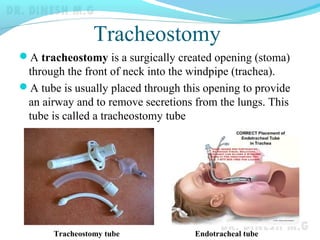
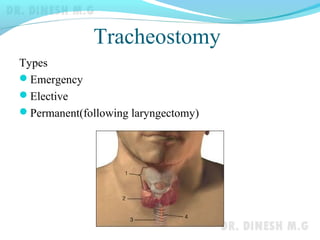
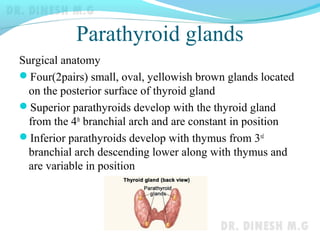




The document discusses tracheostomy, which is a surgically created opening in the neck into the windpipe. A tube is usually placed through this opening to provide an airway and remove secretions from the lungs. Tracheostomies are indicated for upper airway obstruction, retained secretions, or respiratory insufficiency. The procedure involves making an incision below the cricoid cartilage and dividing tracheal rings to insert a tracheostomy tube. Complications can include hemorrhage, injury to nearby structures, or infections. The document also discusses parathyroid glands and hyperparathyroidism.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












