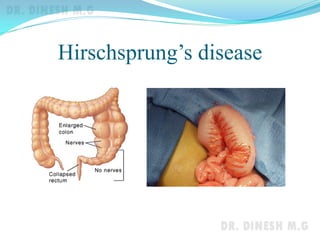
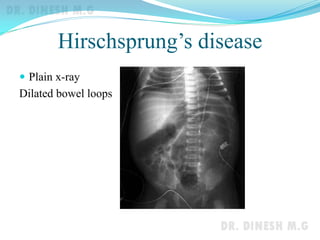
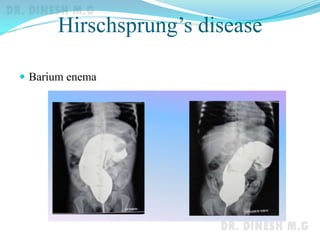
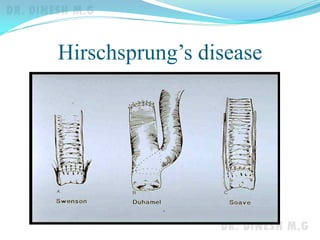


This document discusses Hirschsprung's disease, also known as congenital megacolon. It is a congenital disorder characterized by the absence of ganglion cells in the distal colon, resulting in functional obstruction. The pathology involves absent ganglion cells in the anorectum extending variably upwards. Clinical features include failure to pass meconium in newborns and chronic constipation in older children. Diagnosis is confirmed by full thickness rectal biopsy showing absent ganglion cells. Surgical treatment involves excision of the aganglionic segment and anastomosis of the healthy colon to the anorectum.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















