Imperforate anus is a birth defect where the rectum is malformed, causing the anus to be missing or narrowed. It occurs in about 1 in 5,000 births. The cause is generally unknown, though some genetic factors are associated. Imperforate anus can occur alone or with other defects as part of a syndrome. Treatment depends on the severity but may involve surgery to open the intestines or repair the anus. Prognosis depends on the type, with low lesions generally having better bowel control outcomes than high lesions.
![Imperforate anus
An imperforate anus or anorectal
malformations (ARMs) are birth defects in
which the rectum is malformed. ARMs are
a spectrum of different congenital
anomalies in males and females which
vary from fairly minor lesions to complex
anomalies.[1] The cause of ARMs is
unknown; the genetic basis of these
anomalies is very complex because of
their anatomical variability. In 8% of
patients, genetic factors are clearly](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-1-320.jpg)
![associated with ARMs.[2] Anorectal
malformation in Currarino syndrome
represents the only association for which
the gene HLXB9 has been identified.[1][3]
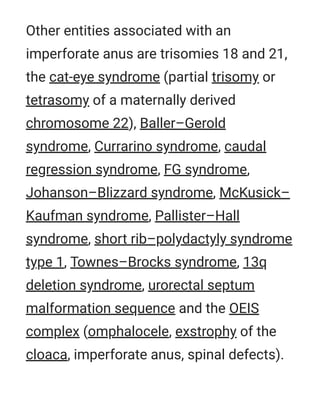
Imperforate anus - Anorectal
malformations
An X-ray showing imperforate anus
Specialty Medical genetics
Features](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-2-320.jpg)
![There are several forms of imperforate
anus and anorectal malformations. The
new classification is in relation of the type
of associated fistula.[4]
The classical Wingspread classification
was in low and high anomalies:
A low lesion, in which the colon remains
close to the skin. In this case, there may
be a stenosis (narrowing) of the anus, or
the anus may be missing altogether,
with the rectum ending in a blind pouch.
A high lesion, in which the colon is
higher up in the pelvis and there is a](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-3-320.jpg)
![fistula connecting the rectum and the
bladder, urethra or the vagina.
A persistent cloaca (from the term
cloaca, an analogous orifice in reptiles
and amphibians), in which the rectum,
vagina and urinary tract are joined into a
single channel.
Imperforate anus is usually present along
with other birth defects—spinal problems,
heart problems, tracheoesophageal fistula,
esophageal atresia, renal anomalies and
limb anomalies are among the
possibilities, collectively being called the
VACTERL association.[5]](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-4-320.jpg)
![usually taken within the first 24 hours of
birth.
Sonography can be used to determine the
type of imperforate anus.[6]
There are other forms of anorectal
malformations though imperforate anus is
most common. Other variants include
anterior ectopic anus.[7] This form is more
commonly seen in females and presents
with constipation.[8]
Variations
Treatment](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-8-320.jpg)
![Imperforate anus usually requires
immediate surgery to open a passage for
feces unless a fistula can be relied on until
corrective surgery takes place. Depending
on the severity of the imperforate, it is
treated either with a perineal anoplasty[9]
or with a colostomy.
While many surgical techniques to
definitively repair anorectal malformations
have been described, the posterior sagittal
approach (PSARP) has become the most
popular. It involves dissection of the
perineum without entry into the abdomen
and 90% of defects in boys can be repaired
this way.](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-9-320.jpg)
![for those with a large rectum, surgery to
remove that dilated segment may
significantly improve the bowel control for
the patient. An antegrade enema
mechanism can be established by joining
the appendix to the skin (Malone stoma);
however, establishing more normal
anatomy is the priority.
Imperforate anus has an estimated
incidence of 1 in 5000 births.[10][11] It
affects boys and girls with similar
frequency.[12] However, imperforate anus
will present as the low version 90% of the
Epidemiology](https://image.slidesharecdn.com/imperforateanus-wikipedia-181129074023/85/Imperforate-anus-11-320.jpg)



















































































