
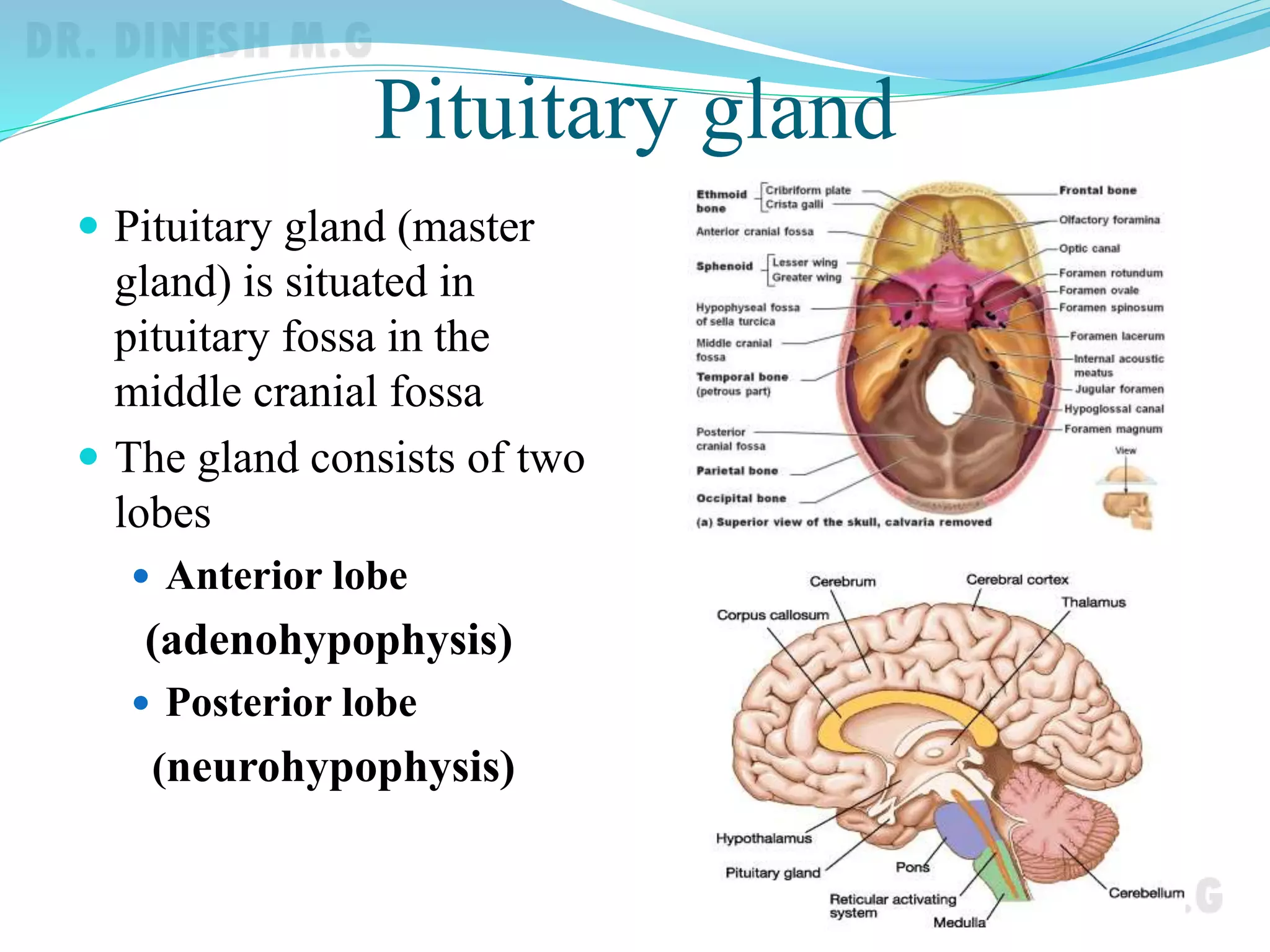



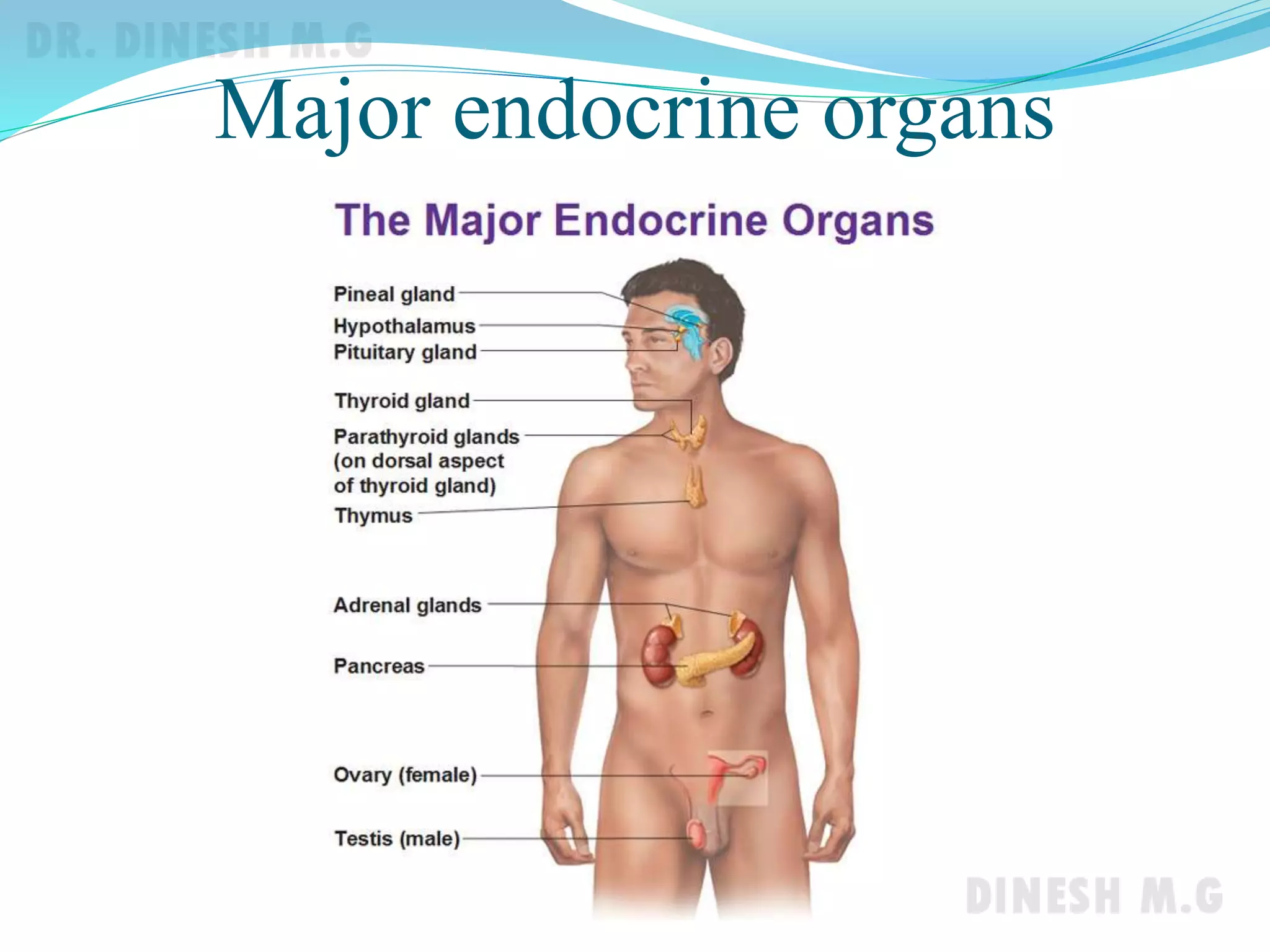






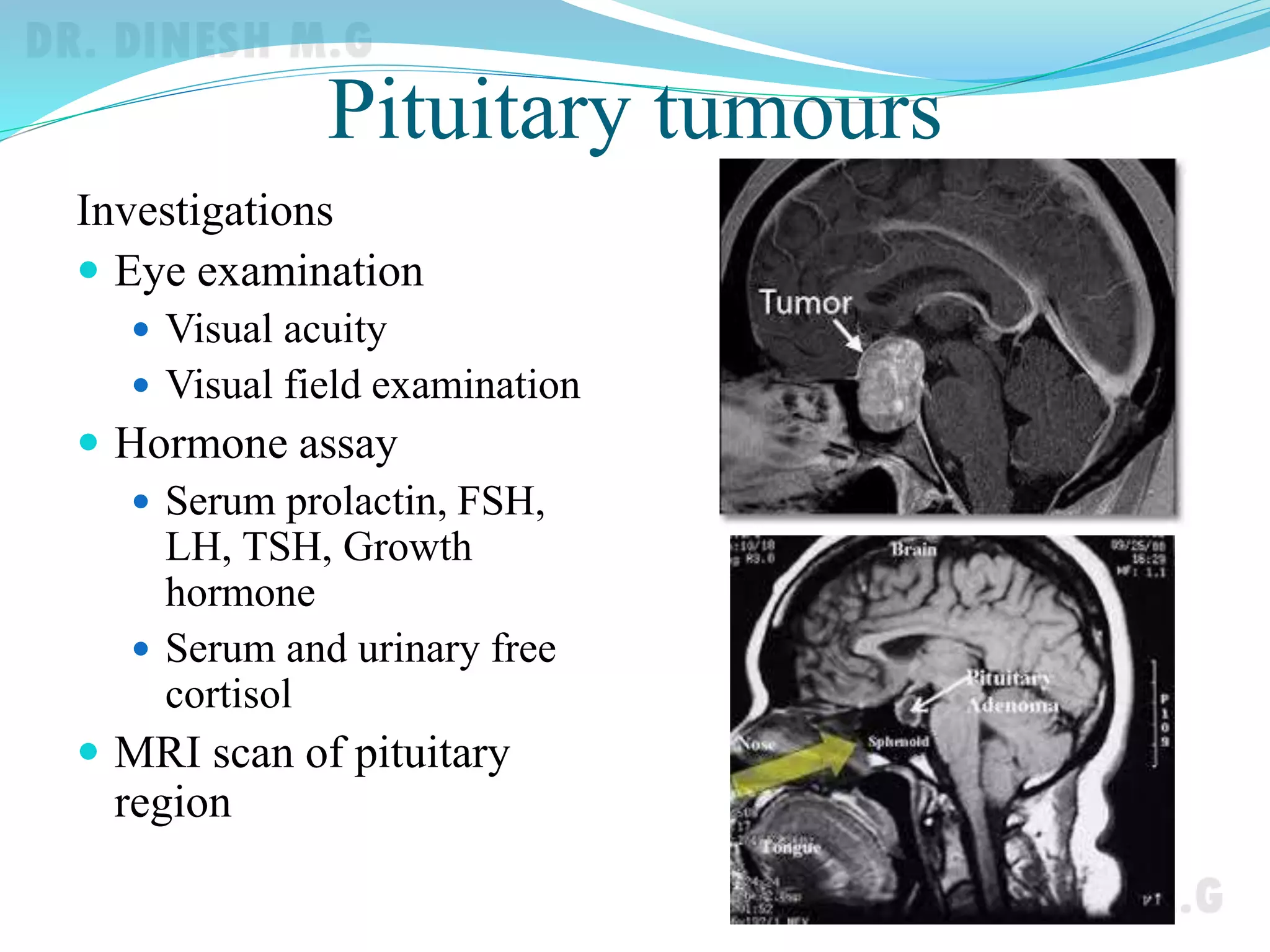




The pituitary gland, also known as the master gland, is located in the sella turcica of the sphenoid bone. It consists of an anterior and posterior lobe. The anterior lobe secretes growth hormone and other hormones that regulate other endocrine glands. The posterior lobe stores and releases oxytocin and antidiuretic hormone produced by the hypothalamus. Diseases of the pituitary gland include hyperpituitarism due to overproduction of hormones and hypopituitarism due to underproduction. Pituitary tumors are also common and can cause hormonal imbalances or pressure effects.























































































