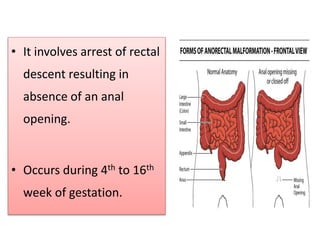
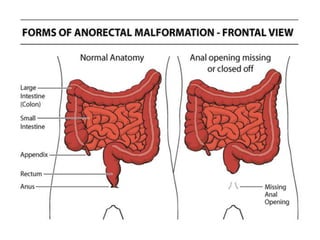
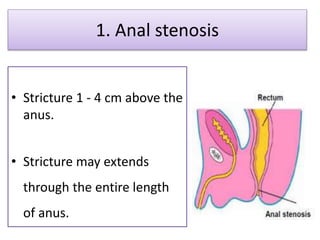
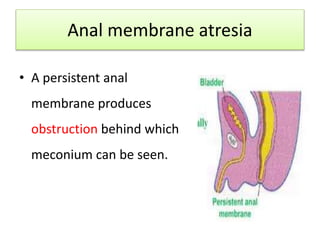
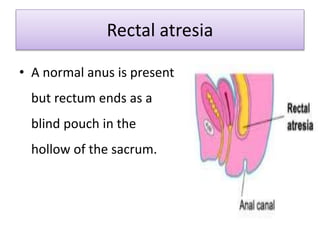
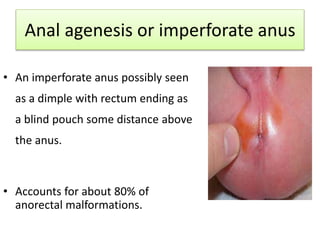
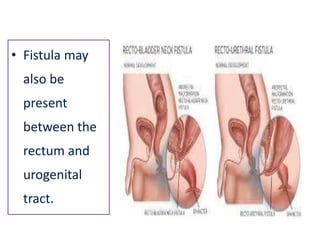





This document discusses anorectal malformations, which involve defects of the distal anus and rectum. It may involve absence of an anal opening. Boys are more commonly affected than girls. Types include anal stenosis, anal membrane atresia, rectal atresia, and anal agenesis. Diagnosis involves newborn assessment and tests like ultrasound and intravenous pyelogram. Surgical procedures depend on the type but may include dilation, incision of membranes, or multi-stage procedures including temporary colostomy. Post-operative nursing care focuses on general care, feeding, and colostomy management if present.



















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


