2. OUTLINE
• Concept
• Embryology and anatomy
• Incidence
• Etiology and classification
• Associated malformations
• Differential diagnosis
• Positive Diagnosis (clinical features, Radiographic studies and other tests)
• Management
•Complication
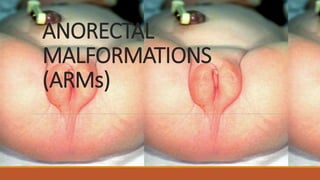
3. CONCEPT
•Anorectal malformations are birth defects that happen as an unborn baby is developing during
pregnancy due to improper development of the rectum and anus
•ARMs comprise a wide range of anomalies that affect boys and girls and can involve the distal
anus and rectum, as well as the urinary and genital tracts.
6. EMBRIOLOGYAND ANATOMY
The hindgut forms early as the part of the primitive gut tube that extends into the tail fold in the
2nd week of gestation
At about day 13, it develops a ventral diverticulum, the allantois or primitive bladder.
The junction of allantois and hindgut become the cloaca, into which the genital, urinary, and
intestinal tubes empty. This is covered by a cloacal membrane.
7. EMBRIOLOGYAND ANATOMY
The urorectal septum descends to divide this common channel by forming lateral ridges, which
grow in and fuse by the middle of the 7th week.
Opening of the posterior portion of the membrane (the anal membrane) occurs in the 8th week.
Failures in any part of these processes can lead to the clinical spectrum of anogenital anomalies.
8. ANATOMY
•The rectum is about 15 cm (6 in.) in length and lies anterior to the sacrum and coccyx. The
terminal 2–3 cm (1 in.) of the large intestine is called the anal canal.
•The mucous membrane of the anal canal is arranged in longitudinal folds called anal columns that
contain a network of arteries and veins.
•The opening of the anal canal to the exterior, called the anus, is guarded by an internal anal
sphincter of smooth muscle (involuntary) and an external anal sphincter of skeletal muscle
(voluntary).
•Normally these sphincters keep the anus closed except during the elimination of feces.
11. ETIOLOGYAND CLASSIFICATION
•There is no known cause for anorectal malformation and most cases are isolated and do run in
families
•According to Krickenbeck classification there are two categories;
1. Based on presence or absence of a fistula
2. Rare or regional variant
12. CLASSIFICATION OF ARMs
1. Major Clinical Groups
Perineal fistula, Rectourethral fistula( Prostatic and Bulbar), Rectovesical fistula, Vestibular fistula,
Cloaca, No Fistula, Anal Stenosis
2. Rare/ regional variants
Pouch Colon, Rectal Atresia/stenosis, Rectovaginal fistula, H-fistula
15. ASSOCIATED MALFORMATIONS
GENITOURINARY
Vesicoureteric reflux, Renal agenesis,
Renal dysplasia, Ureteral duplication,
Cryptorchidism Hypospadias,
Bicornuate uterus Vaginal septums
VERTEBRAL
Spinal dysraphism, Tethered chord,
Presacral masses, Meningocele,
Lipoma, Dermoid, Teratoma
CARDIOVASCULAR
Tetralogy of Fallot, Ventricular septal
defect, Transposition of the great
vessels, Hypoplastic left heart
syndrome
GASTROINTESTINAL
Tracheoesophageal fistula Duodenal
atresia, Malrotation Hirschsprung ’ s
disease
CENTRAL NERVOUS SYSTEM
Spina bifida, Tethered cord
16. ASSOCIATED MALFORMATIONS
CON’T
When the diagnosis of ARM is made, the child should therefore be examined for other components of
the VATERR OR VACTERL complex of anomalies
VATERR - vertebral, anal, tracheal, esophageal, radial, renal
VACTERL - Vertebral and spinal cord, Anorectal, Cardiac, Tracheo-Esophageal, Renal and other
urinary tract, Limb
18. CLINICAL FEATURES
Patients present in 2 groups:
A. Those without obstruction – Usually in females
B. Those with obstructive symptoms
(i) No meconium is passed from birth. Vomiting is rather late and the abdomen is distended.
Such patients may have anorectal agenesis without fistula, complete anal membrane or rectal
atresia.
(ii) Small amounts of meconium are passed, but the baby is distended and may vomit. The cause
may be anorectal agenesis with a narrow fistula, perineal or vestibular fistula with a narrow
opening, or anorectal stenosis
19. CLINICAL FEATURES
All neonates should be carefully examined at birth for any anomalies.
Where an anorectal anomaly is suspected, the perineum, vulva, vagina, scrotum and penis should
be well inspected for any
A. Small opening
B. Skin folds
C. Meconium staining
D. A bulge of an anal membrane
20. CLINICAL FEATURES CON’T
A flat perineum without an anal dimple suggests that the anomaly is probably high.
An anal dimple suggests a low anomaly.
Meconium may be seen through the skin suggesting a perineal fistula if it is outside of the anal
region, and a membrane if it is at the expected site of the anus.
21. RADIOLOGICAL STUDIES
Abdominal ultrasound to examine genitourinary tract.
An X-ray of the lateral view of the baby head-down with a radio-opaque marker on the anal
dimple and the X-ray tube centered on the greater trochanter is taken(cross table lateral x ray)
If the lower end of the gas shadows is within 1cm of the marker then primary repair may be done
without colostomy. If it is 1 cm then the anomally is most probably a high one
(b) Any sacral or lumbar abnormality is noted.
Colostography is done later in those with a colostomy to find the lower end of the colonic pouch
and if there is a fistula.
Cardiac Echocardiogram is important to rule out any congenital heart lesion.
22. Sickling status
Full blood count
Blood urea and electrolytes
Urinalysis
Imaging:
abdominopelvic ultrasound to examine the
genitourinary tract.
contrast X-ray(cross table lateral X-ray)
23.
24. OTHER TESTS
FBC
Sickling and BUE
Urinalysis is done if meconium has not been detected during examination. Meconium in the urine
confirms recto-urinary fistula.
25. MANAGEMENT
The ultimate aim is to repair any defects and restore the anus to its normal anatomical site within
the external sphincter using the posterior sagittal anorecloplasty (PSARP) method
After physical and imaging assessment, patients fall into 2 main groups:
I. Those in whom primary repair can be done
2. Those who require sigmoid colostomy first and repair later.
Anal Membrane: This is incised and dilation of the anus performed.
Anorectal Stenosis: Daily dilatation is required
26. COMPLICATIONS
• lncontinence especially in high anomalies is a problem.
• Stenosis or stricture at the muco-cutancous junction after abdominal pull-through may occur.
Dilatation is performed.
• Prolapse of mucosa may occur and must be excised.
27. REFERENCE
• Ascraft Paediatric Surgery
• Baja Surgery
• Nelson Paediatrics
• Paediatric Surgery: Comprehensive text
• Gerard J. Tortora / Bryan Derrickson: Principles of anatomy & physiology