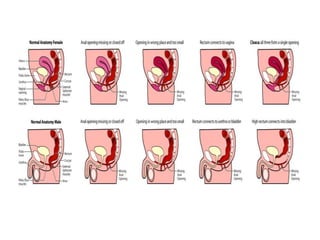
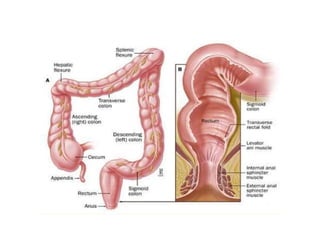
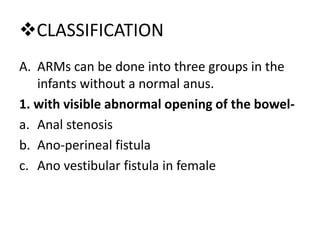
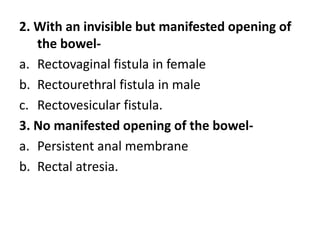
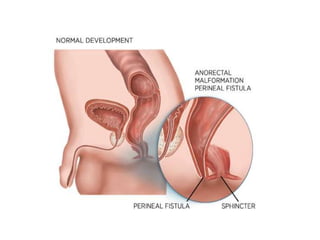
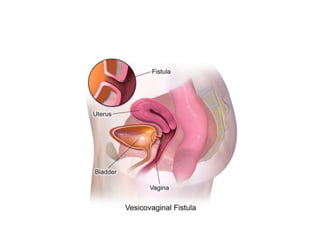
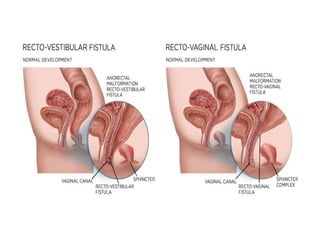
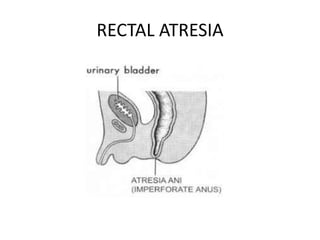
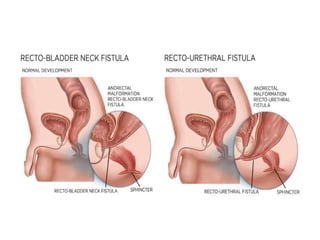
This document discusses anorectal malformations, which are developmental deformities of the lower end of the alimentary tract that occur due to arrest in embryonic development. Anorectal malformations can be classified into three main groups based on whether there is a visible abnormal opening, invisible opening, or no opening. They can also be classified based on where the rectum terminates in relation to the levator ani muscle. Clinical manifestations include abnormal or no anal opening and absence of passing meconium. Diagnosis involves physical examination, imaging tests, and urine/stool examinations. Management involves reconstructive surgery such as rectal anoplasty or initial colostomy followed by definitive surgery later.