Downloaded 73 times
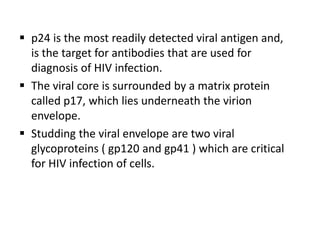
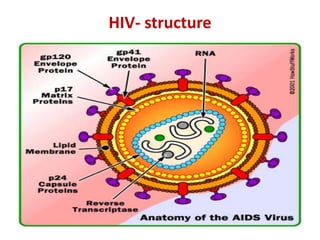
![Secondary[Acquired]
Immunodeficiency states](https://image.slidesharecdn.com/immunopathology-5-130219045932-phpapp01/85/Immunopathology-5-1-320.jpg)
![Secondary[Acquired]
Immunodeficiency states](https://image.slidesharecdn.com/immunopathology-5-130219045932-phpapp01/75/Immunopathology-5-1-2048.jpg)


This document summarizes secondary immunodeficiency states and acquired immunodeficiency syndrome (AIDS). It describes AIDS as being caused by the human immunodeficiency virus (HIV) which leads to immunosuppression and opportunistic infections. The virus is transmitted through unprotected sex, blood transfusions, from mother to child, and sharing of infected needles. HIV infects immune cells like CD4+ T cells and macrophages. This results in loss of CD4+ T cells and ultimately immune system failure putting individuals at risk for infections and cancers.


































































![Prac excises 3[1].5](https://cdn.slidesharecdn.com/ss_thumbnails/pracexcises31-150331131154-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)













