Downloaded 618 times
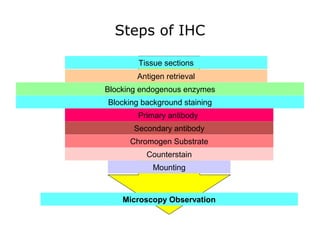
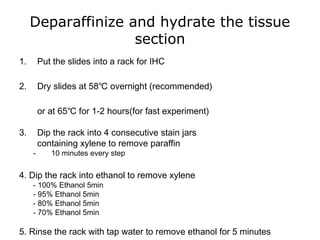
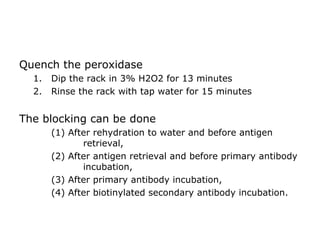
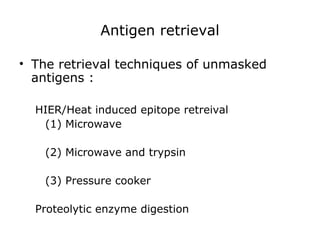


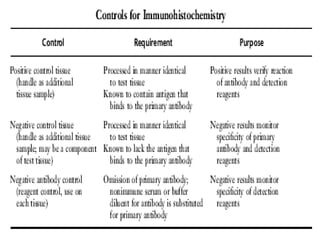
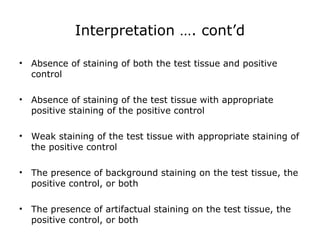





















This document provides information on immunohistochemistry (IHC), including: 1. IHC is used to detect antigens in tissues through antigen-antibody recognition at the light microscopic level. It applies immunologic principles and techniques to study cells and tissues. 2. The basic principle of IHC is a sharp visualization of target components in cells and tissues based on a satisfactory signal-to-noise ratio. 3. The main steps of IHC are tissue processing, antigen retrieval, primary/secondary antibody incubation, detection, counterstaining, and mounting. Proper controls and interpretation of results are also discussed.


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



