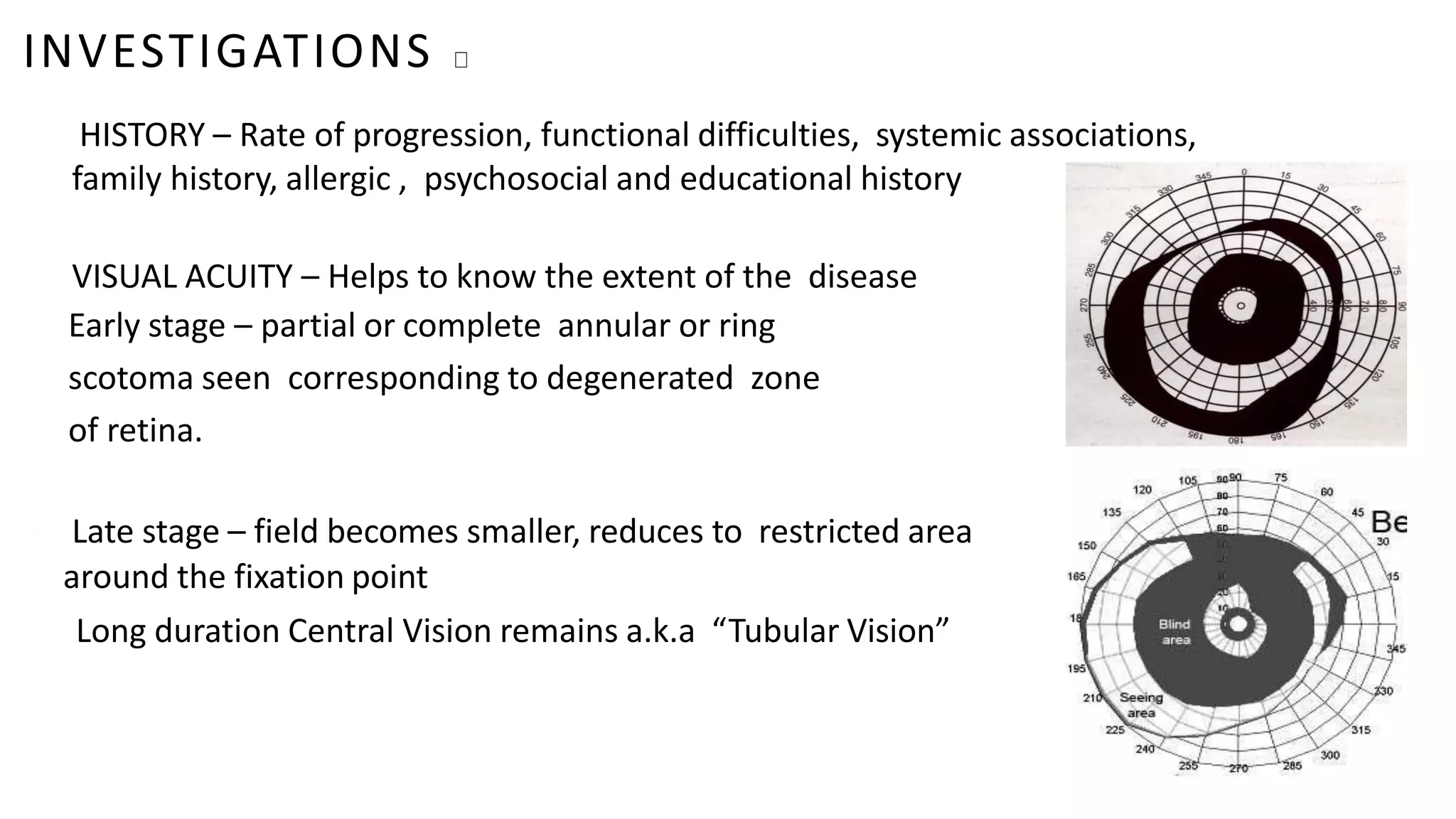
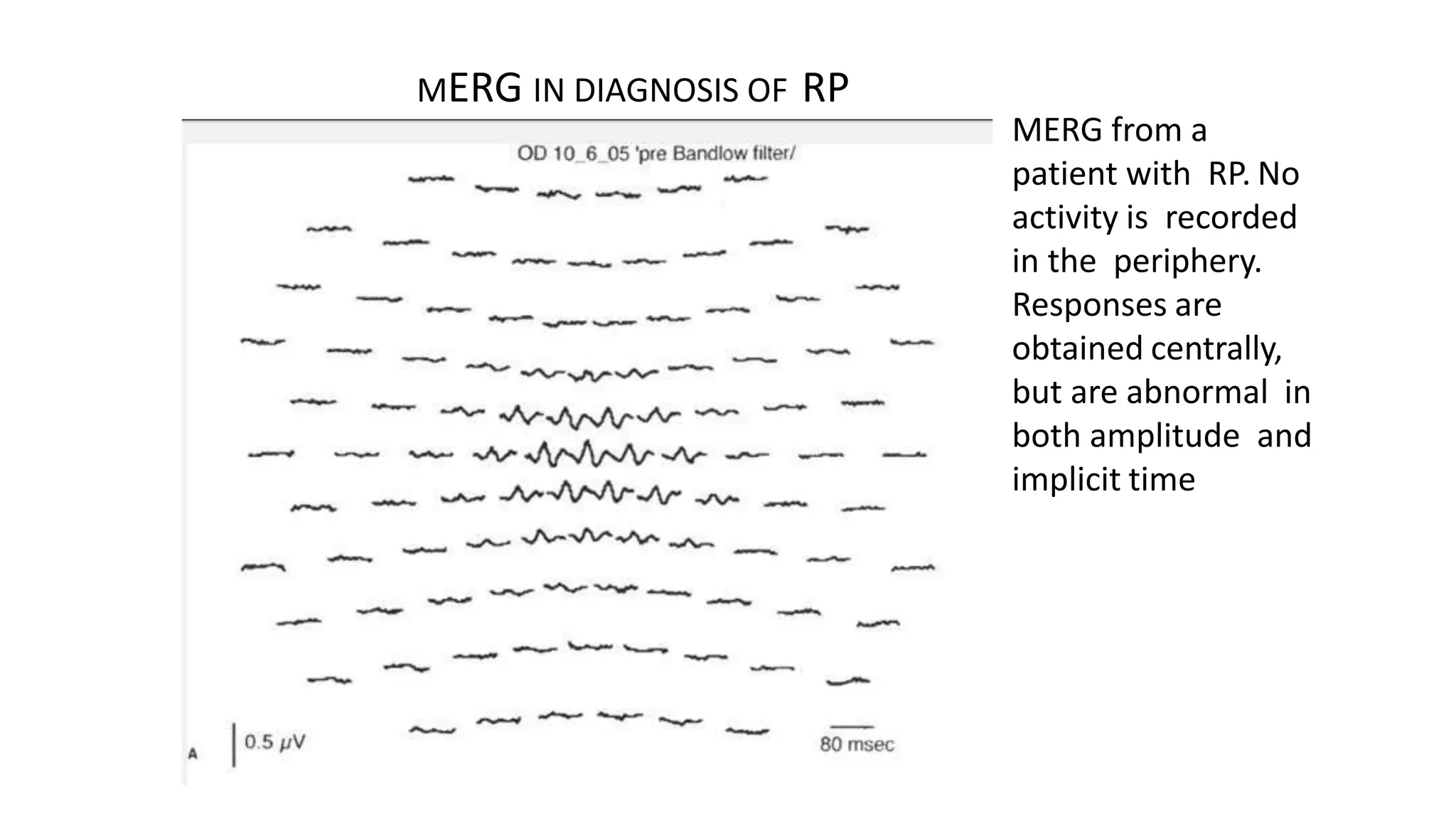
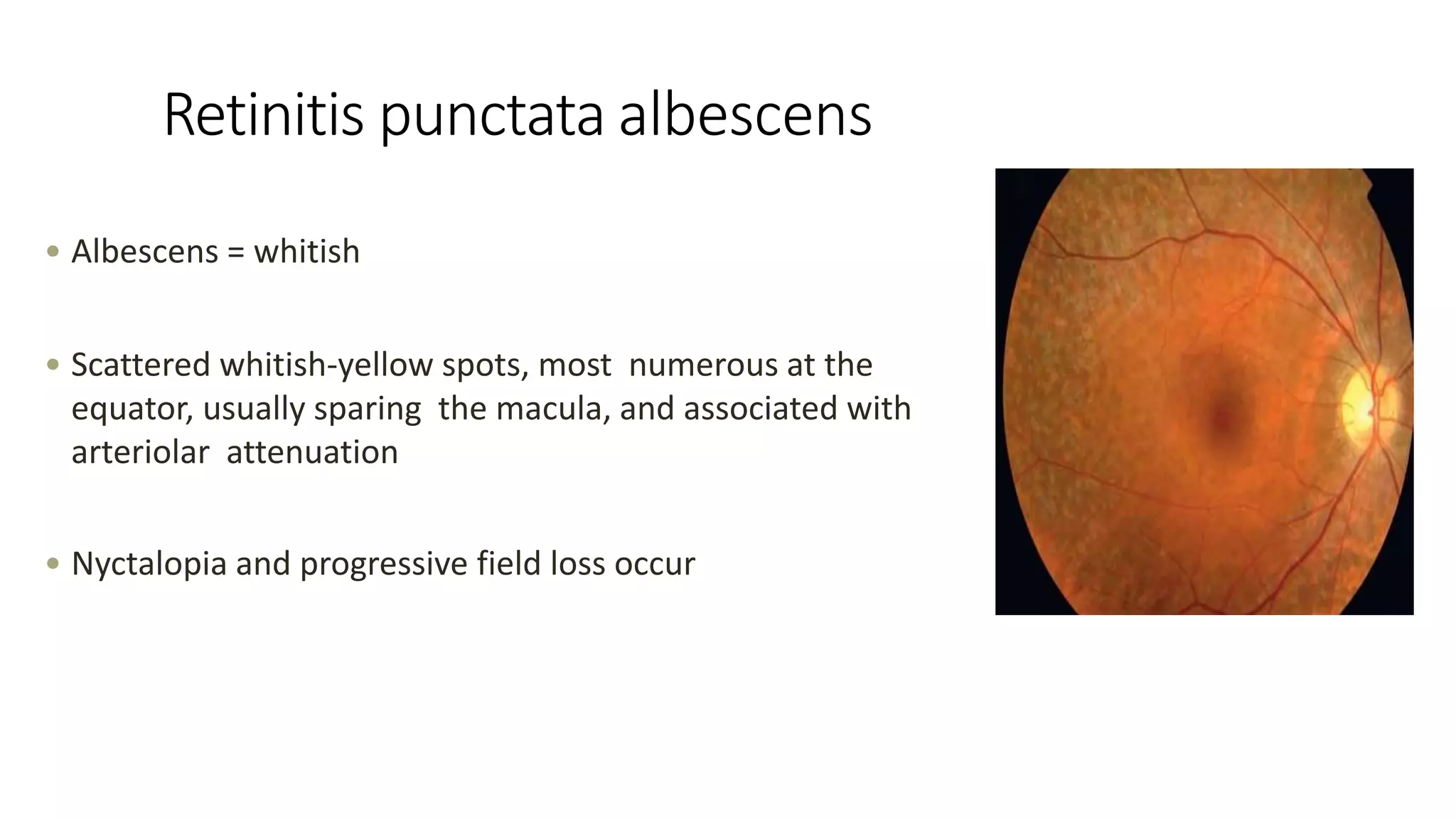
Retinitis pigmentosa is a group of inherited retinal diseases characterized by progressive vision loss. It has a prevalence of 1 in 3500 people. The document discusses the various types of retinitis pigmentosa based on inheritance patterns and symptoms. It also summarizes the clinical features, investigations, management, and associated syndromes of retinitis pigmentosa.