Download to read offline
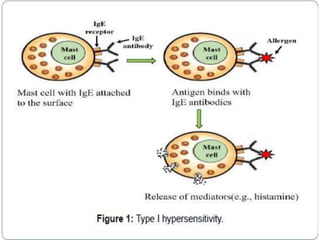
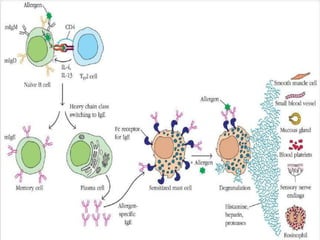
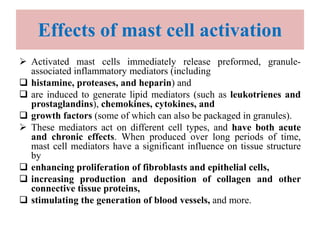
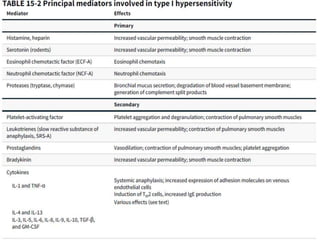
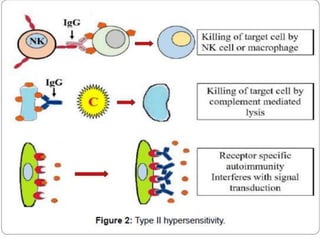

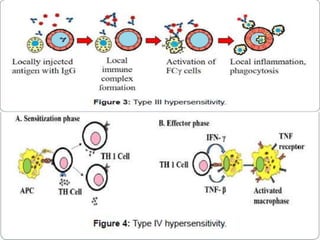
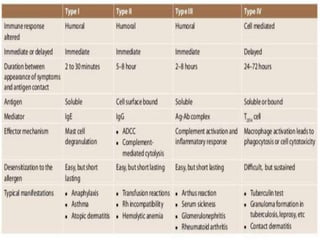

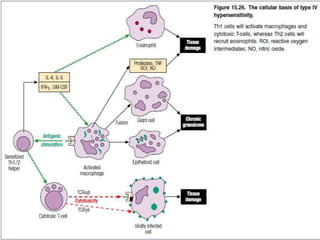

Hypersensitivity reactions are harmful immune responses that occur on reexposure to an antigen. There are four main types of hypersensitivity reactions: Type I reactions are mediated by IgE antibodies and include allergic responses. Type II reactions involve IgG/IgM binding to host cells marking them for destruction. Type III reactions occur when antigen-antibody complexes activate complement or induce inflammatory mediator release. Type IV reactions are T cell-mediated and cause delayed hypersensitivity responses like contact dermatitis.




















































































