Downloaded 150 times

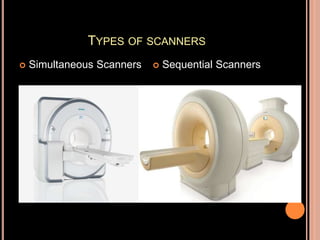
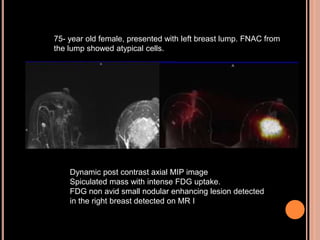
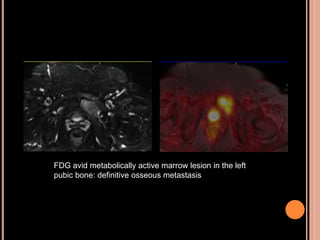
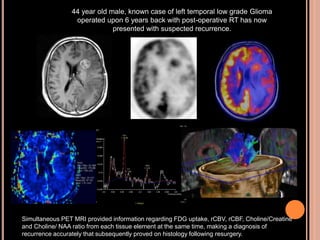

PET-MRI is a hybrid imaging technique that was approved by the FDA in 2011. It provides both the anatomical details from MRI and the functional and metabolic information from PET. There are two main types of PET-MRI scanners: simultaneous and sequential. Implementation of PET-MRI presents challenges related to PET detector elements, attenuation correction, and system corrections. PET-MRI shows potential for use in neurology, oncology, pediatrics, cardiology, and musculoskeletal imaging by providing more biological and functional data than PET-CT without radiation exposure. Examples of clinical applications include detecting tumor recurrence, evaluating treatment response, and replacing painful bone marrow biopsies for lymphoma.




















































![Pet mr poster-4-15-2012_v2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pet-mrposter4-15-2012v21-120417090725-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Pet mr poster-4-15-2012_v2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pet-mrposter4-15-2012v21-120521081020-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)