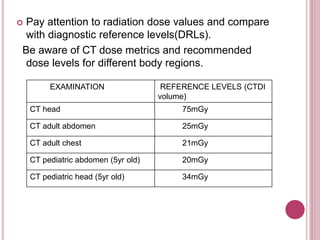
This document discusses various techniques for reducing radiation dose in computed tomography (CT) scans. It outlines strategies such as using automatic exposure control, adjusting scan parameters based on patient size, employing noise-tolerant images when possible, limiting scan lengths and phases, and utilizing newer reconstruction techniques. The goal is to lower radiation dose without compromising diagnostic image quality.