Downloaded 56 times
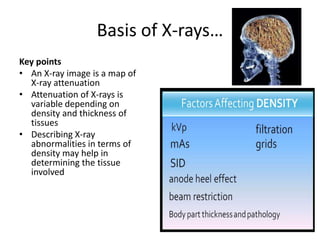
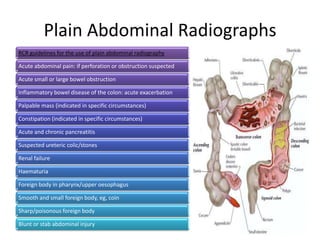



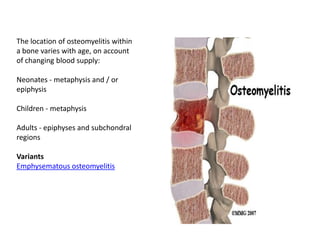
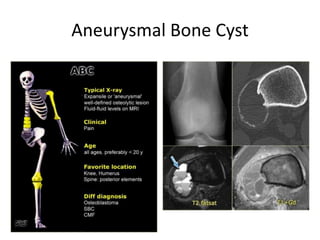
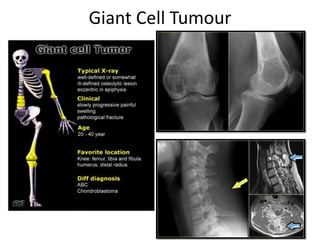






This document provides an overview of various radiographic findings related to the chest, abdomen, bones, and arthritis. Key points include: - X-ray attenuation depends on tissue density and thickness, and abnormalities can be described based on density. - Chest X-rays should be requested if bowel perforation is suspected to look for signs like Rigler's sign or the football sign. - Abdominal X-rays can help identify bowel obstruction or inflammation. Findings include bowel dilation and loss of haustral markings. - Osteomyelitis appears as bone destruction, periosteal reaction, and new bone formation. Location varies by age. - Bone tumors like aneurysmal bone cyst, ench























































































