Download as PDF, PPTX




































































































































































































































































































































































































































































































































































































































































This document discusses the levels of organization in the human body from cells to organisms. It defines key terms like cells, tissues, organs, and organ systems. It explains that cells make up tissues, tissues make up organs, and organs work together in organ systems. Some key organ systems mentioned are the digestive system, circulatory system, and respiratory system. The relationship between cells, tissues, organs, systems and organisms is illustrated through a flow chart. The document provides a high-level overview of the hierarchical structure of the human body.
Introduction to human anatomy and levels of organization from cells to organisms.
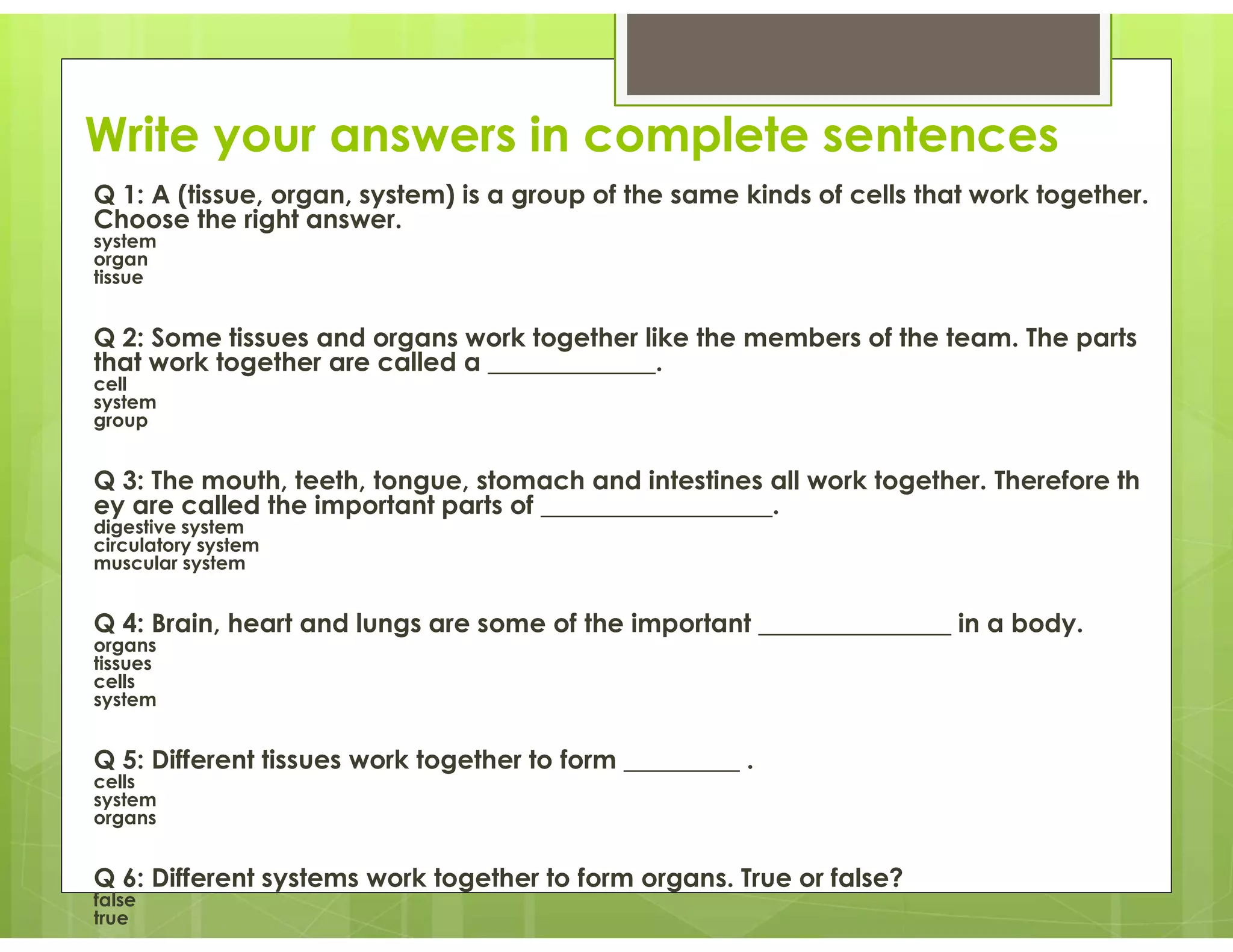
Explains hierarchical structure: cells, tissues, organs, organ systems, and organisms.
Covers human organ systems, their types, and major organs involved.
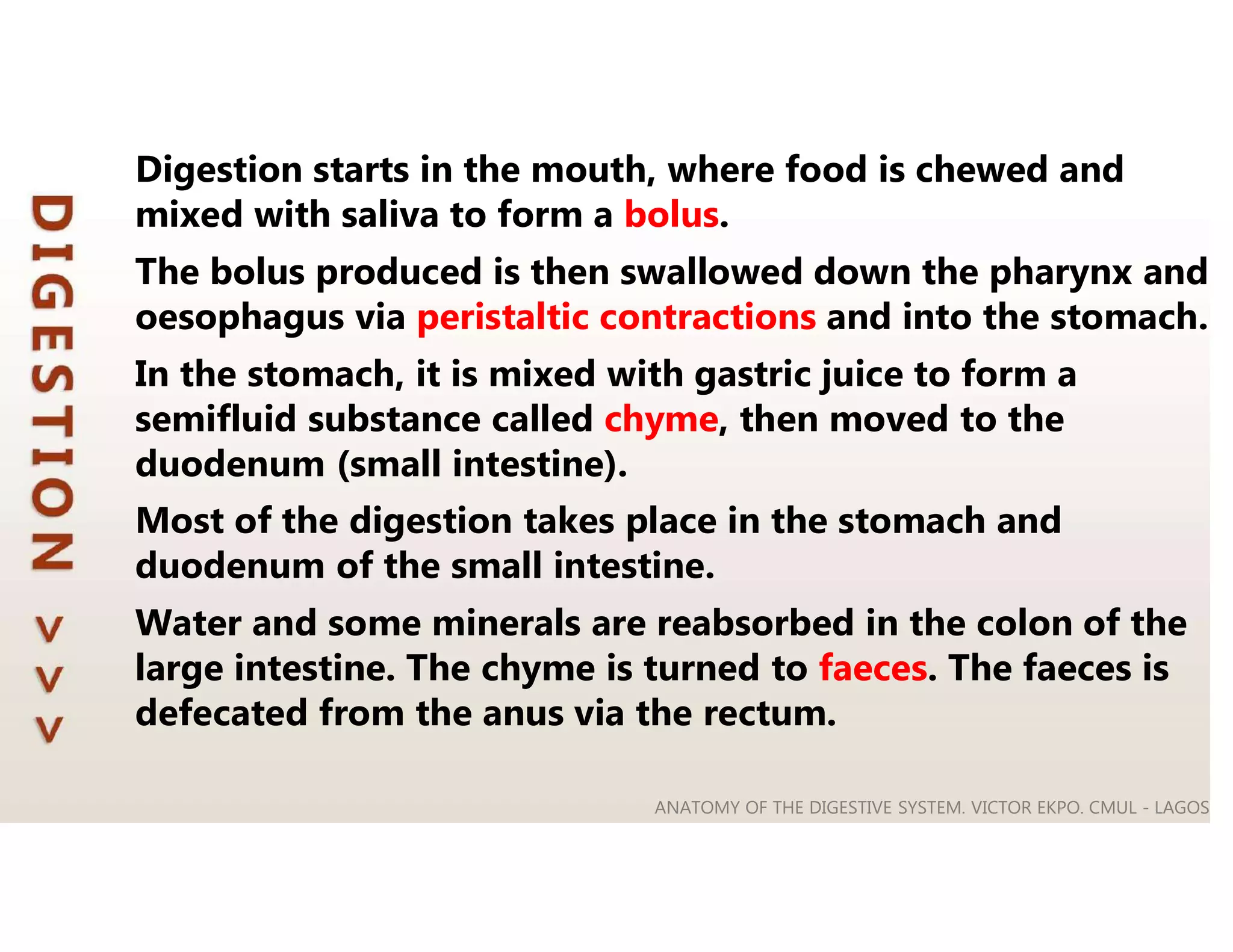
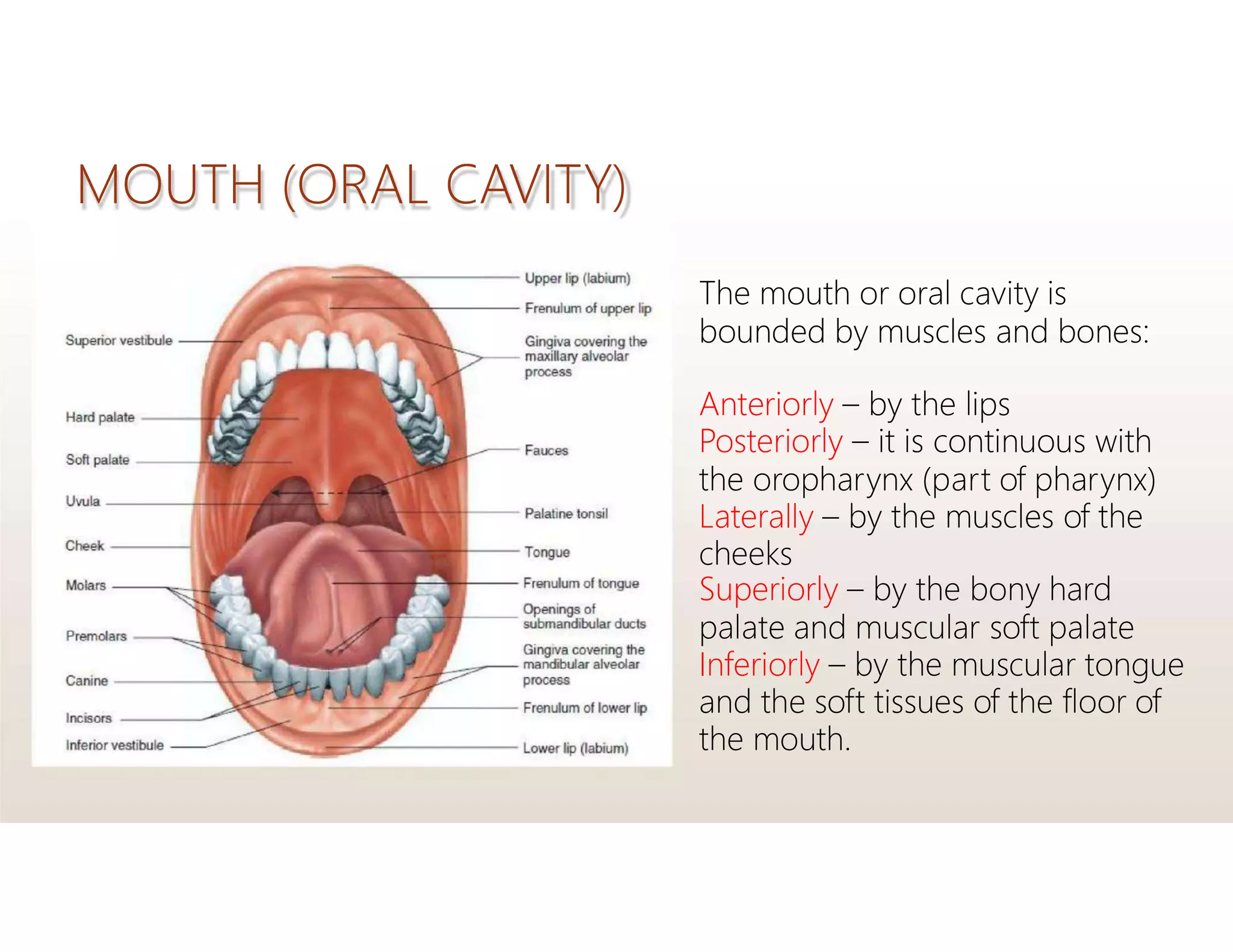
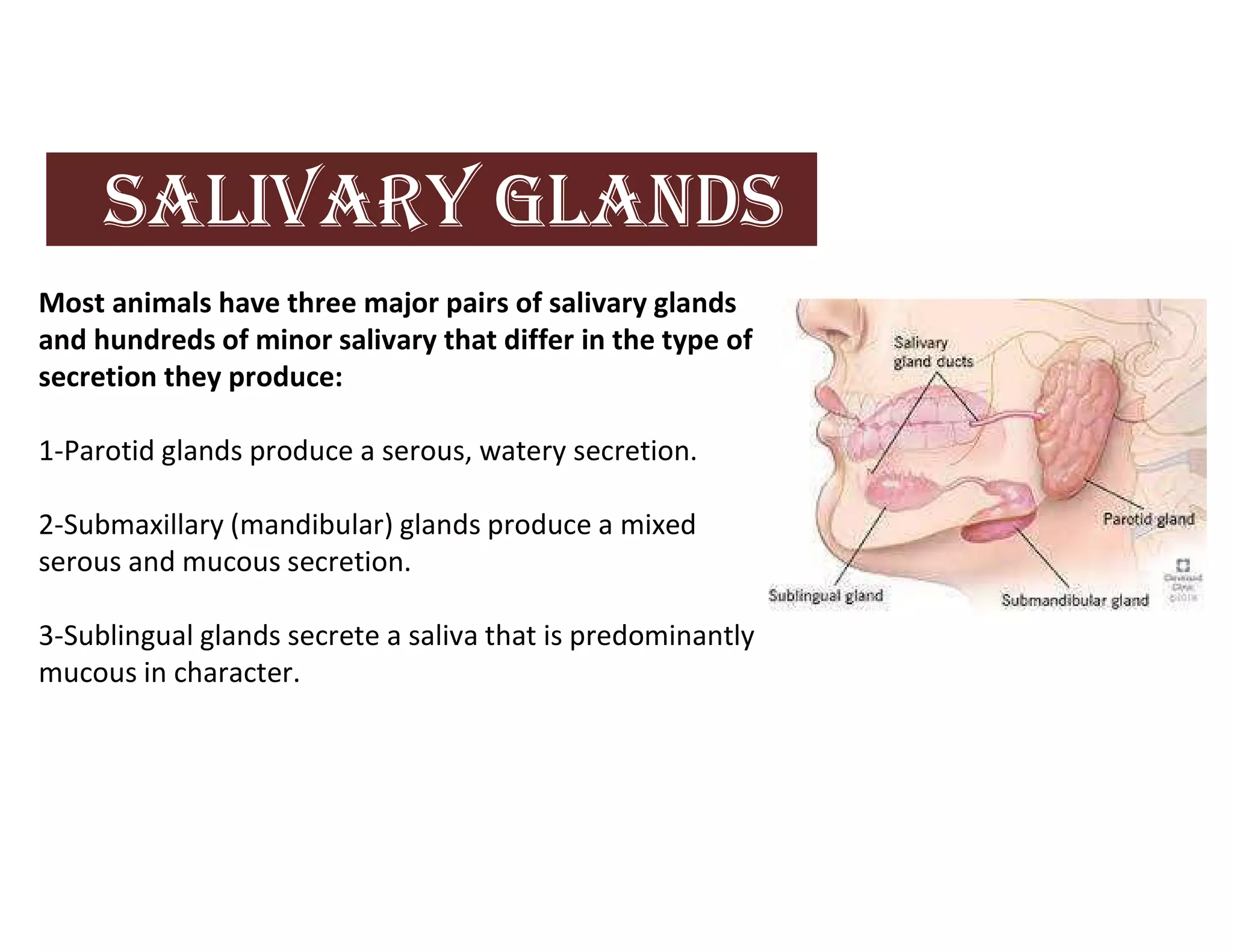
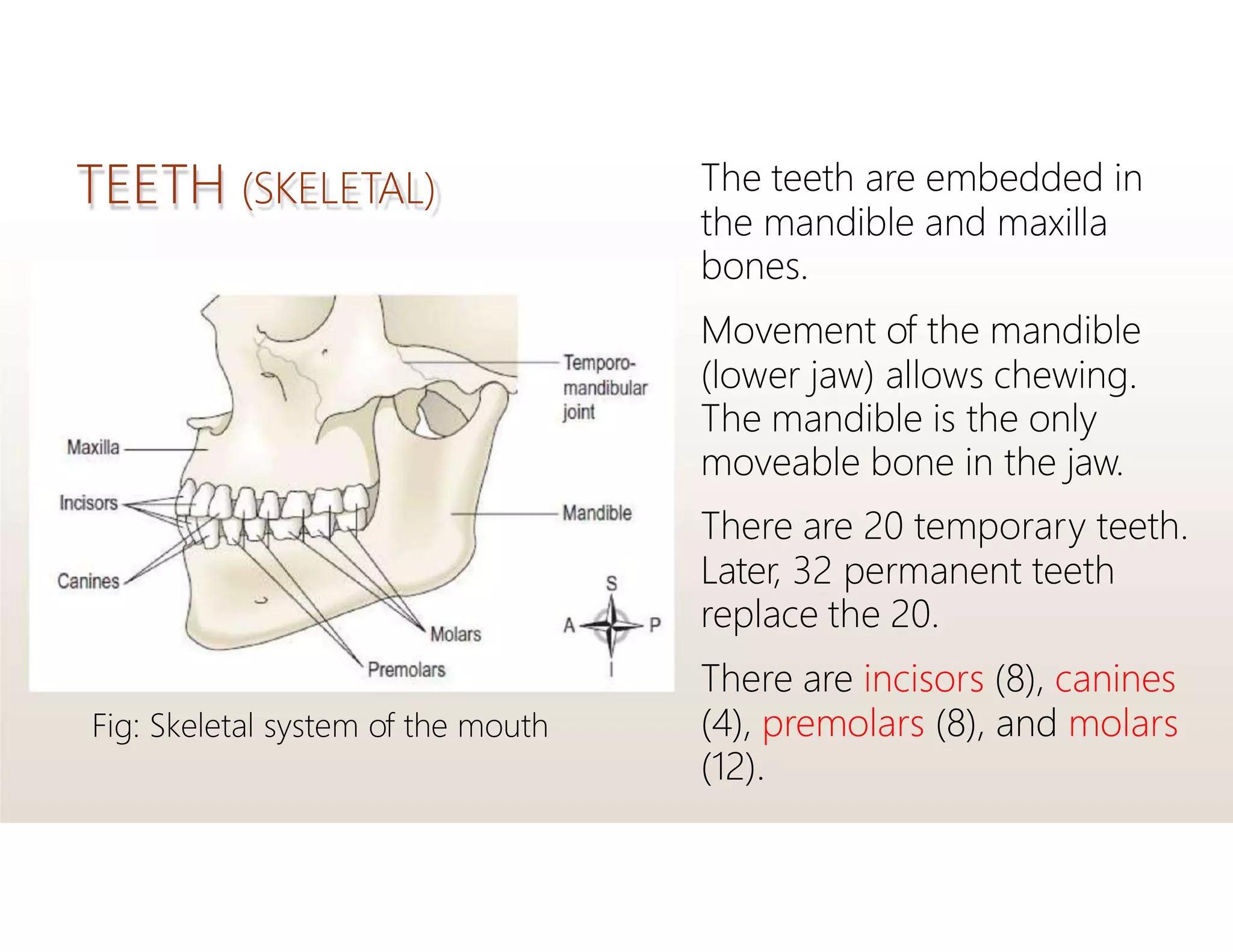
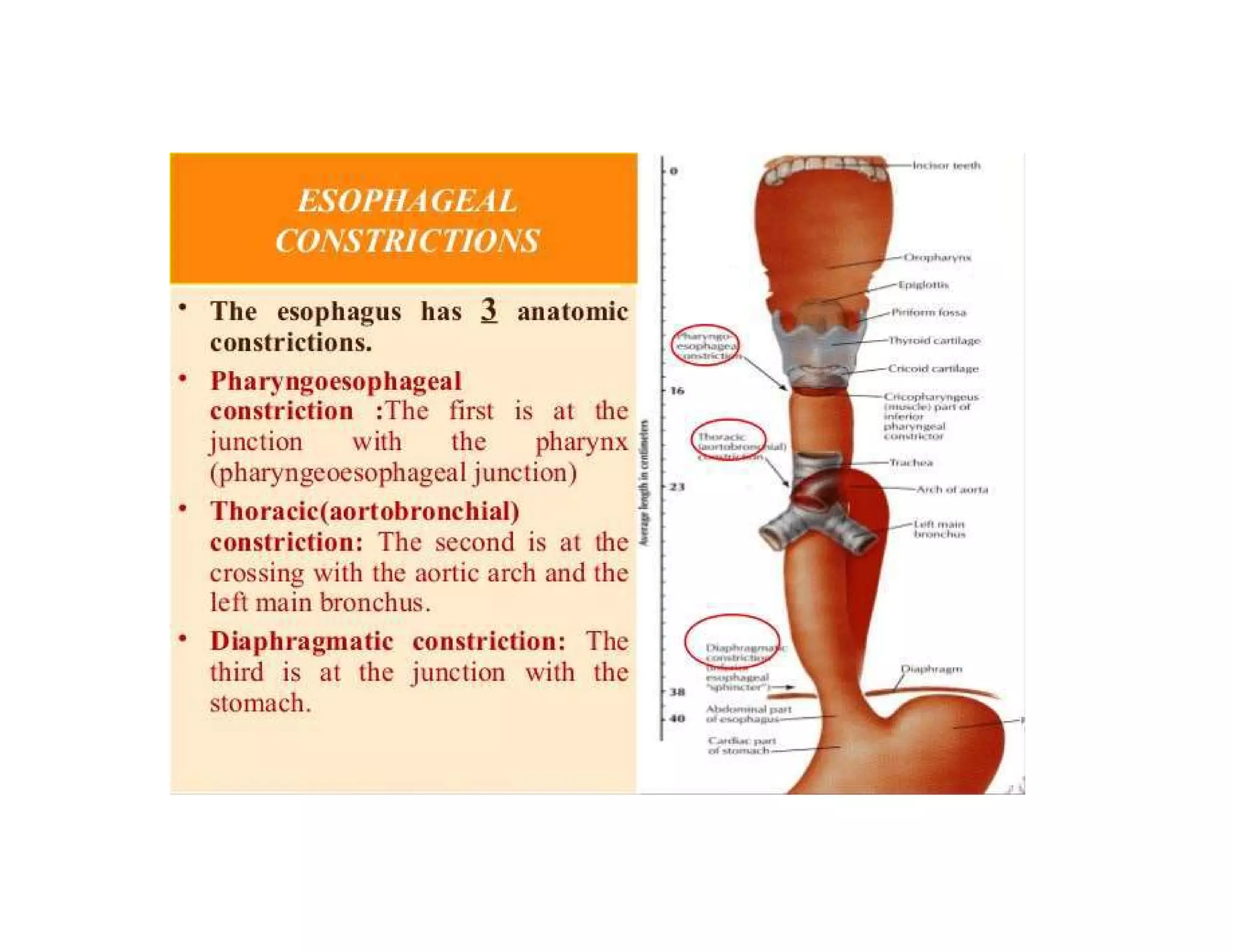
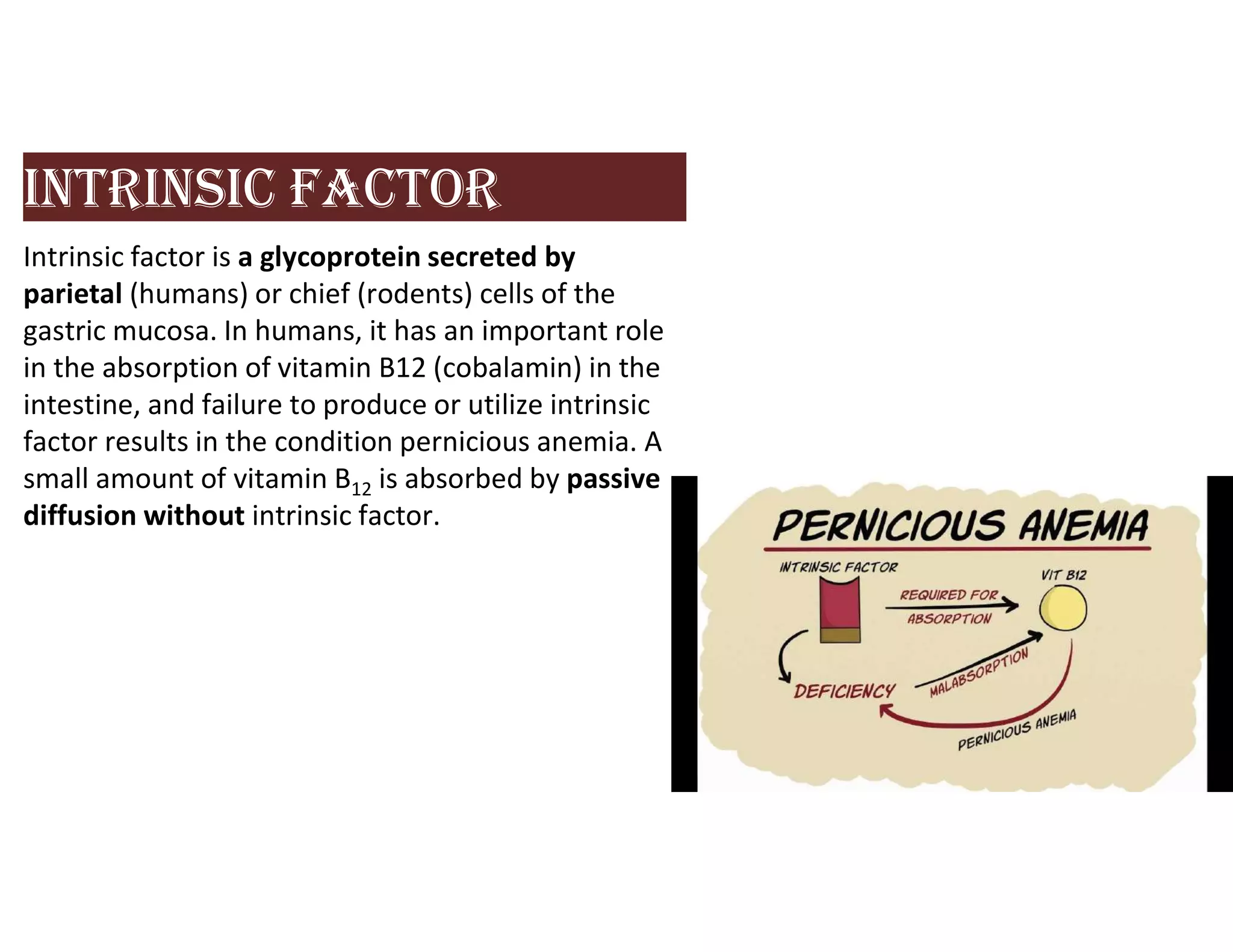
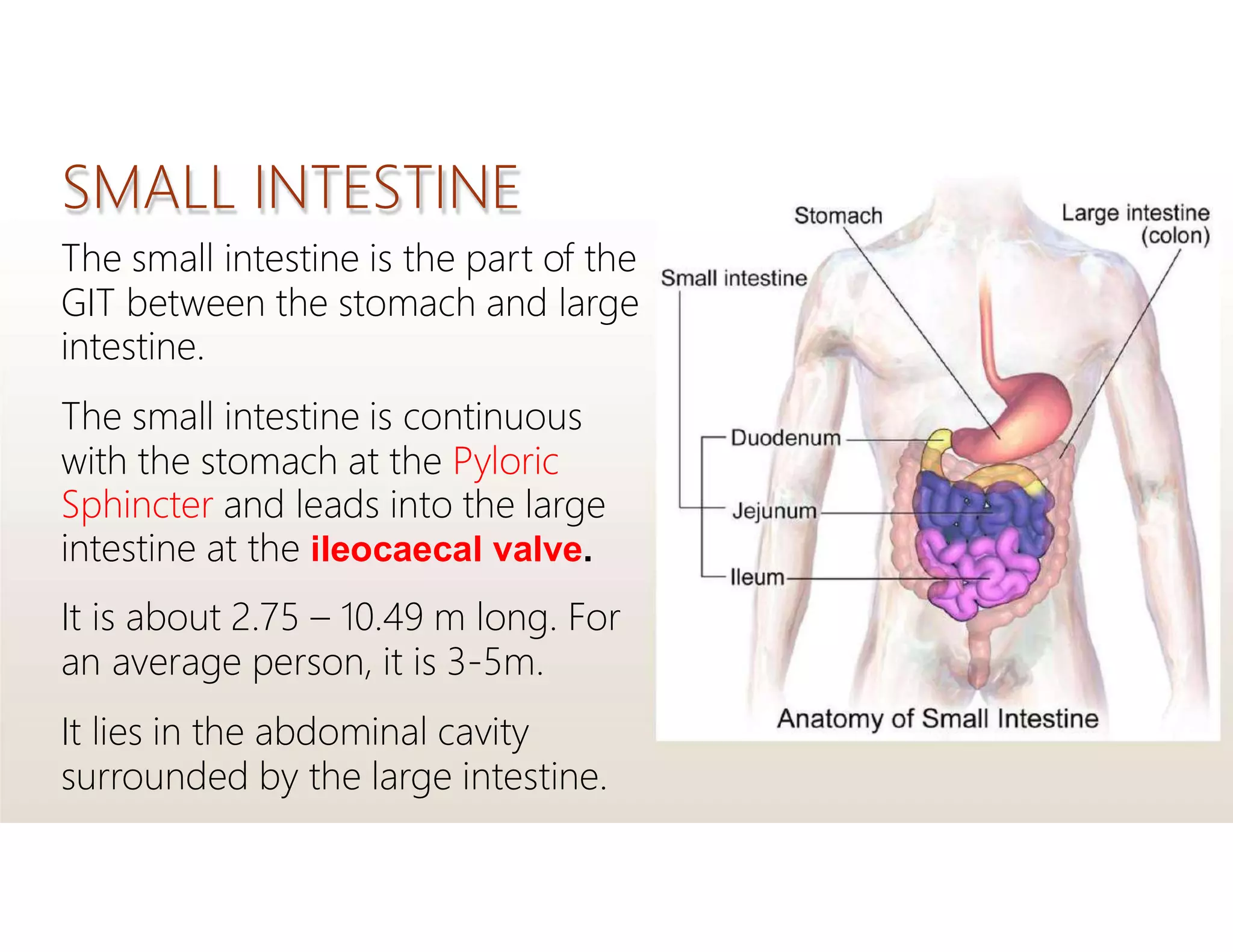
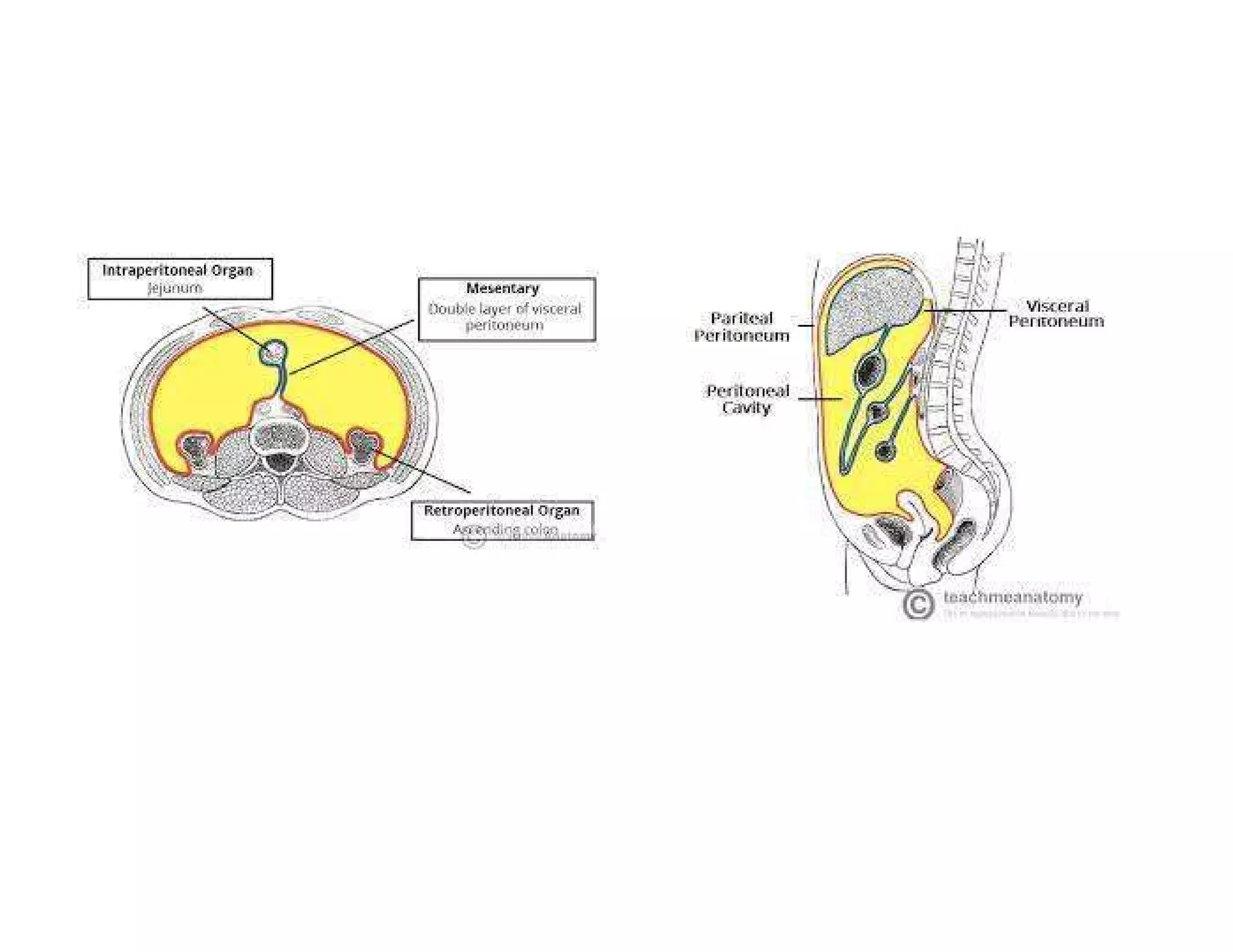
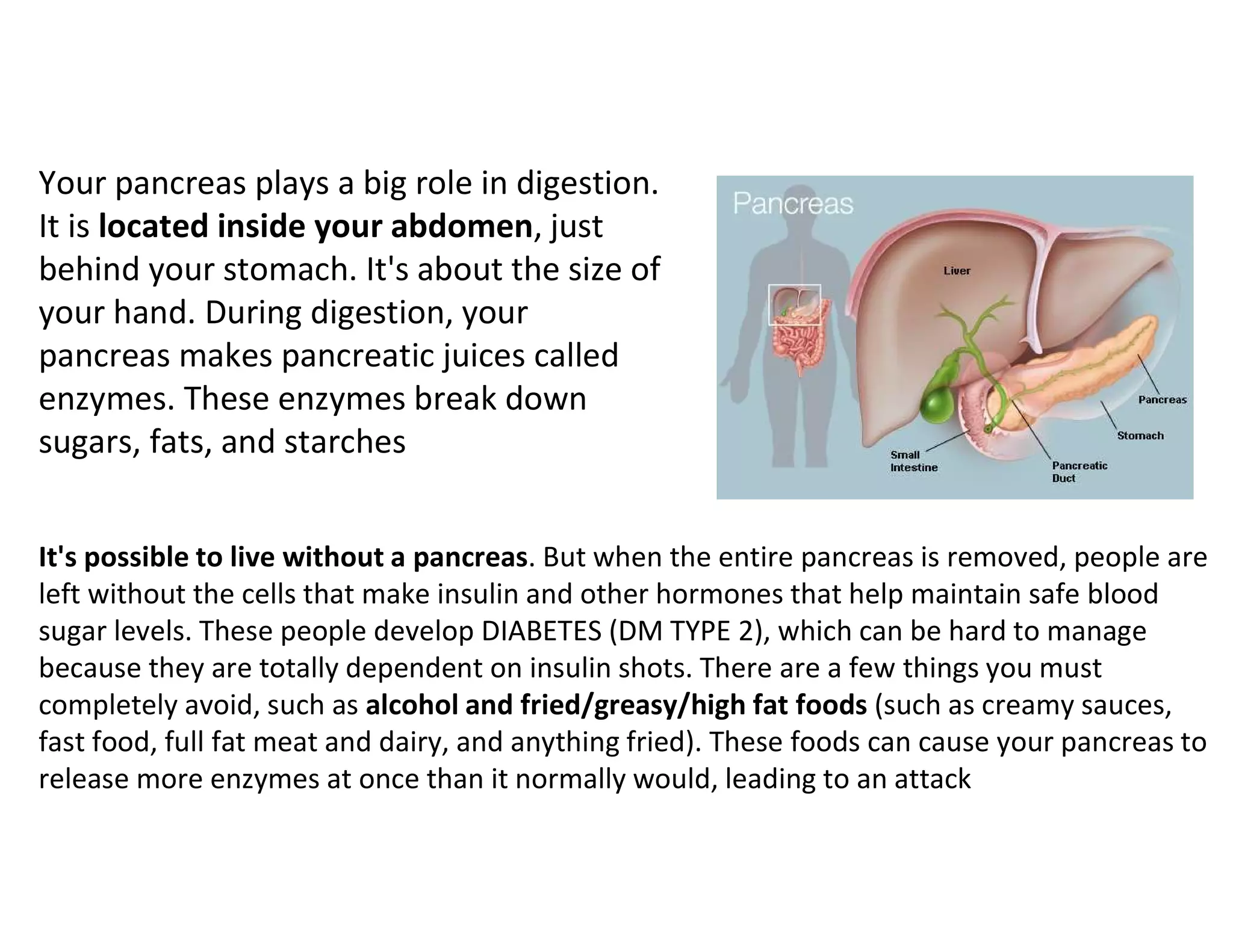
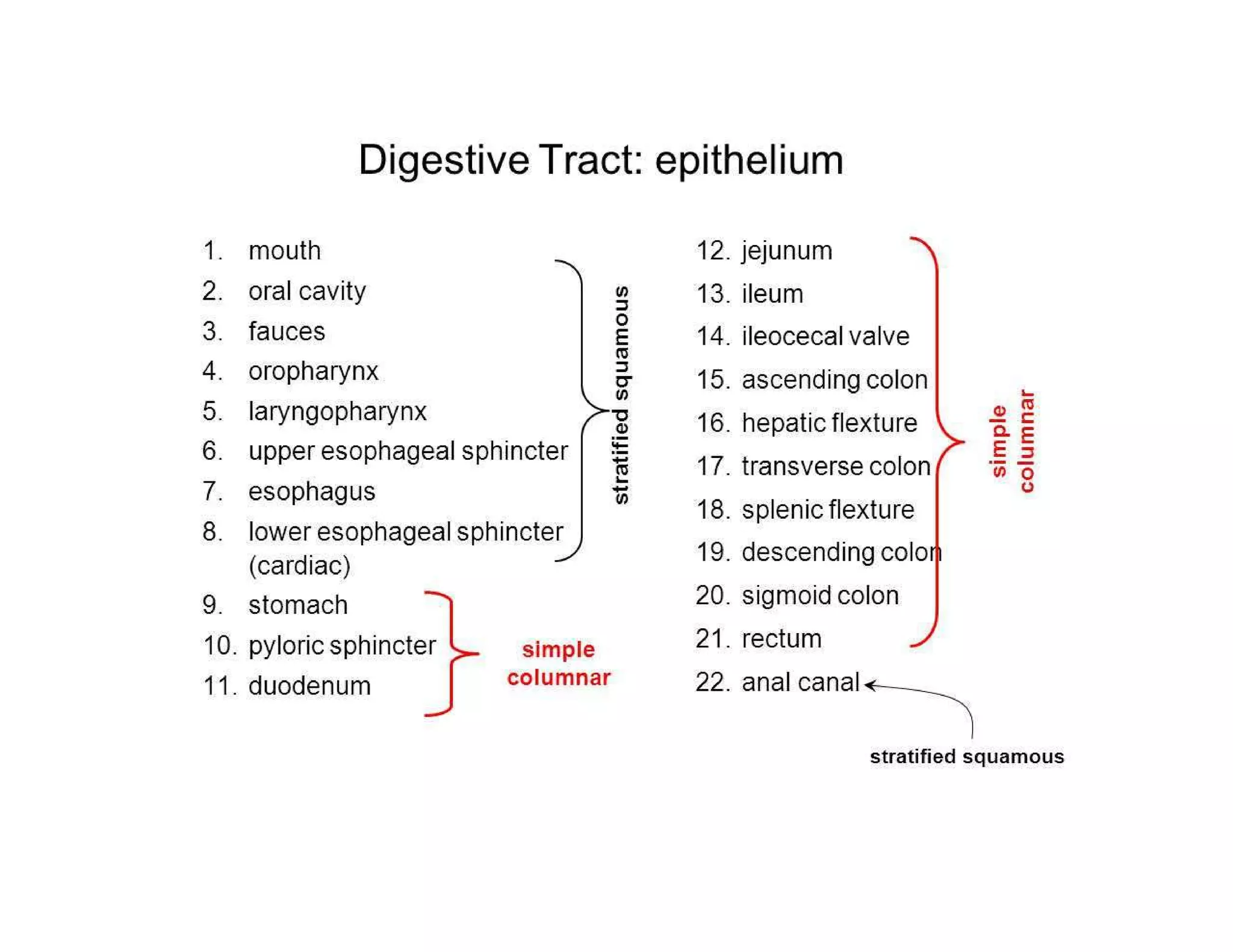
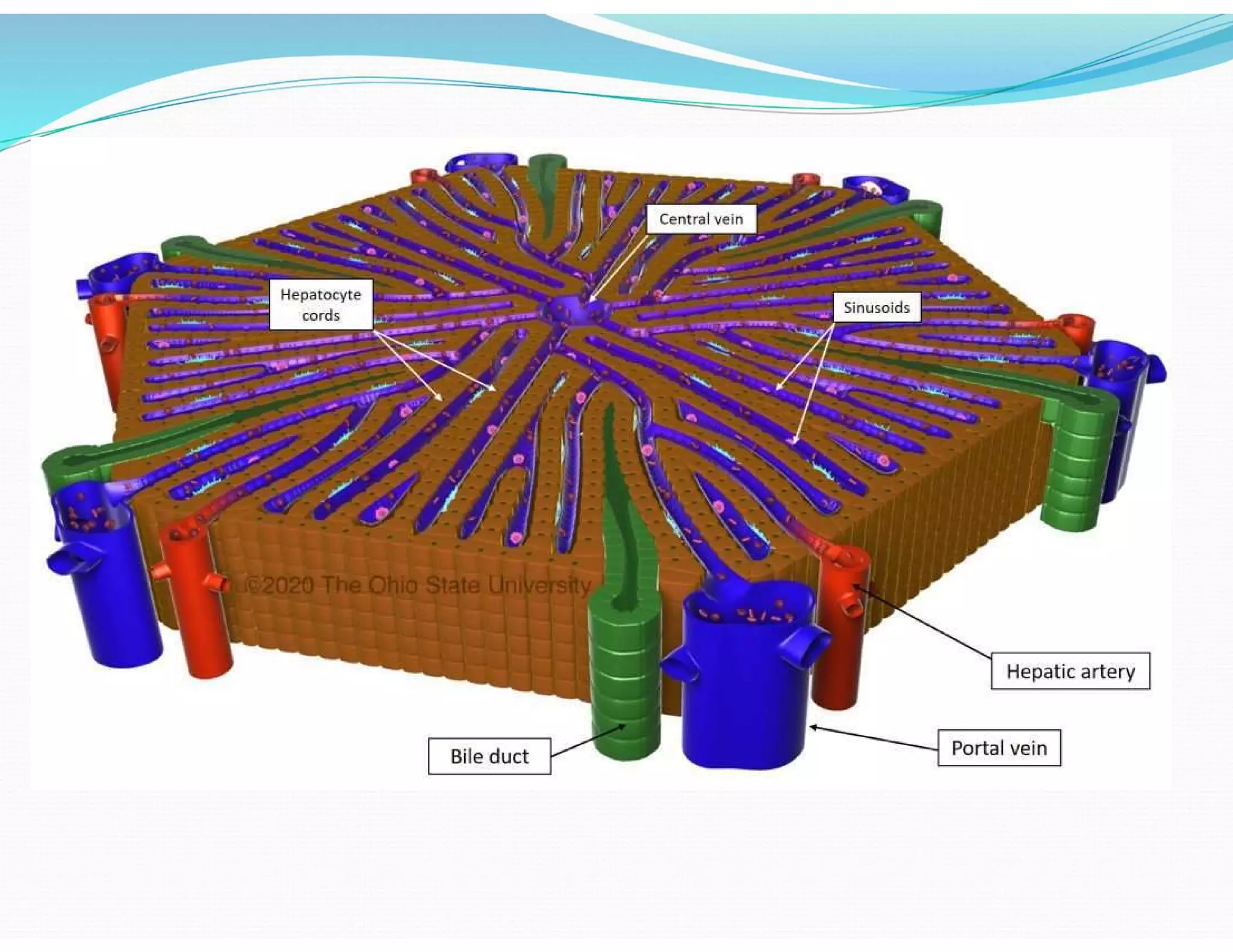
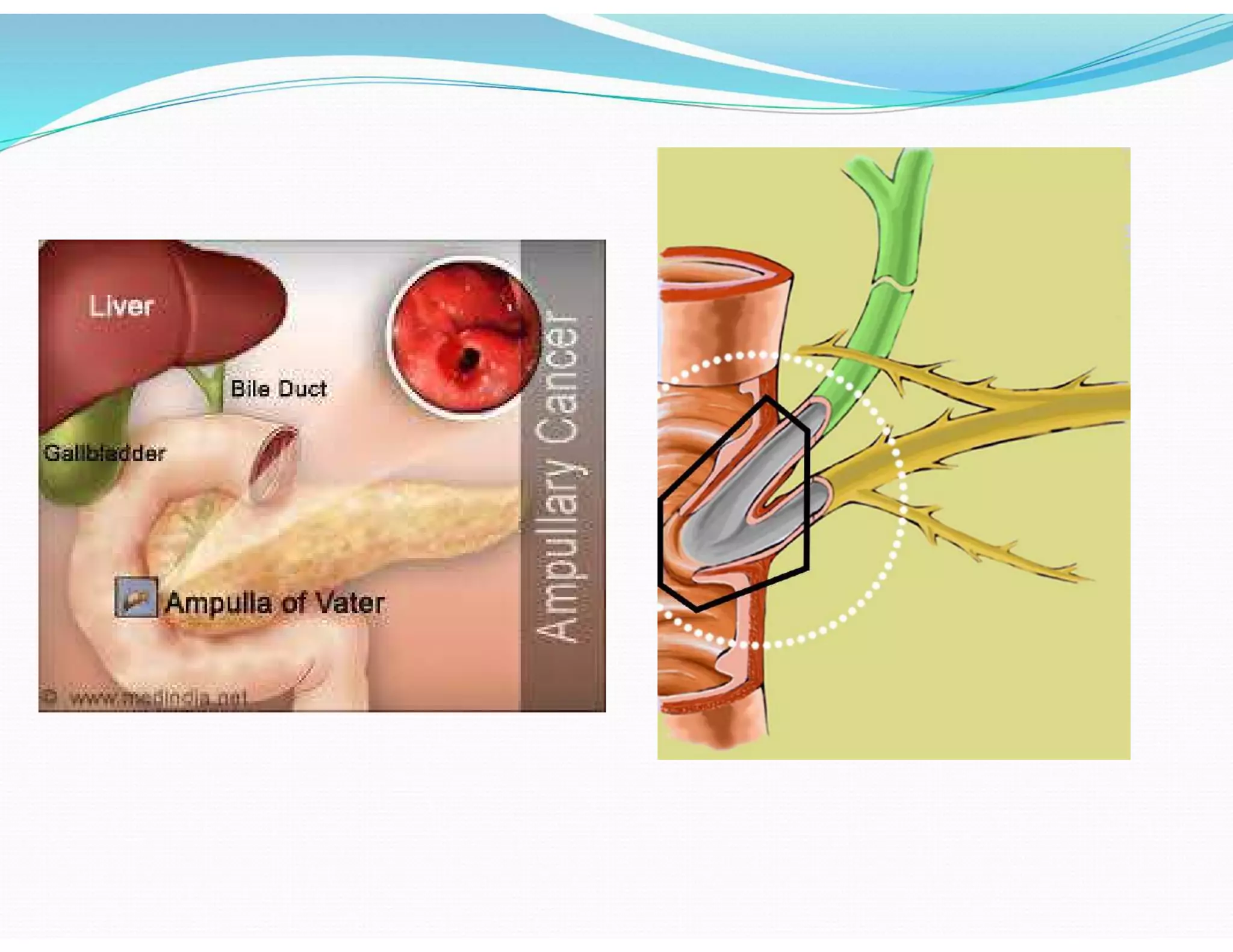
Details on the digestive system, its organs, functions, and connections.
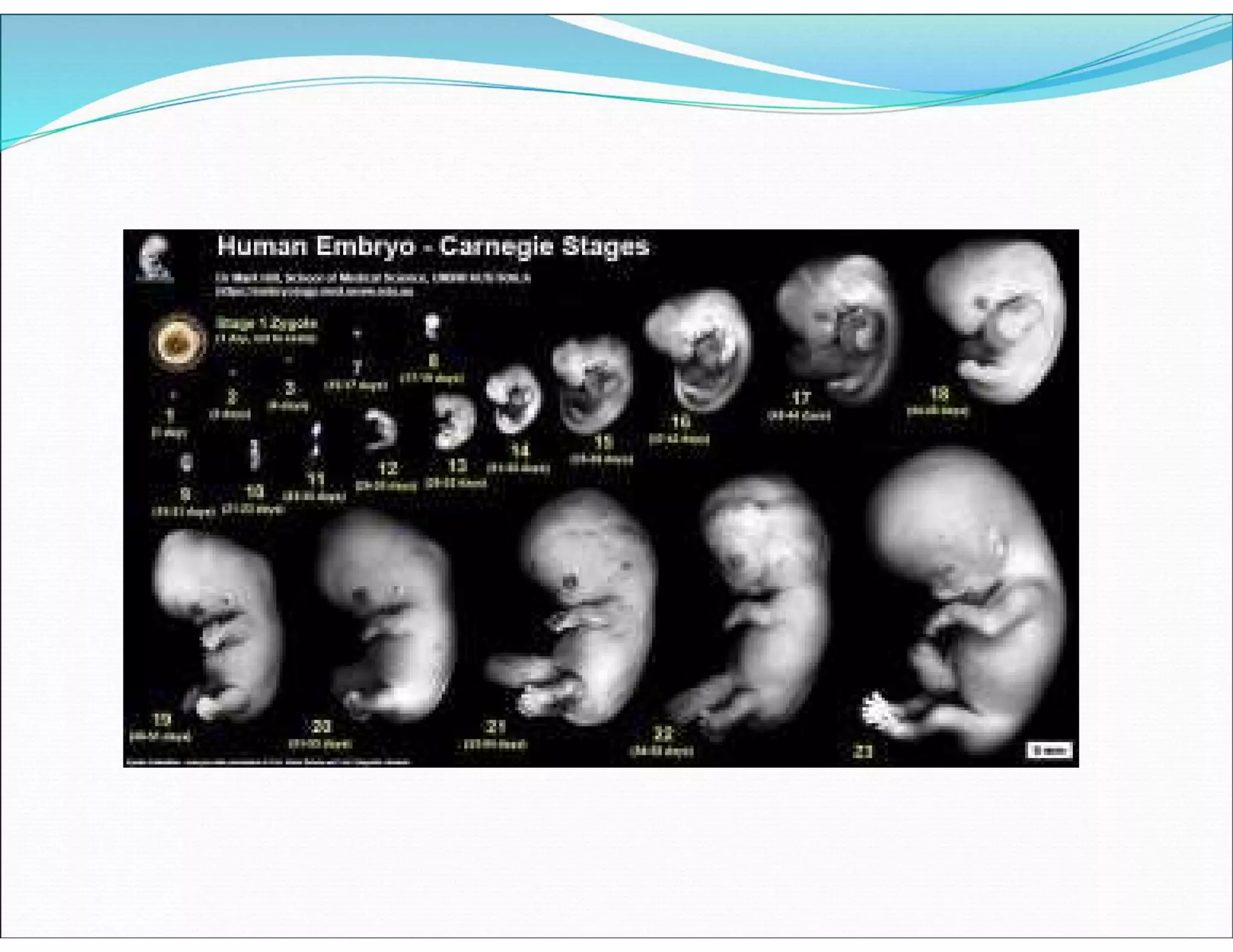
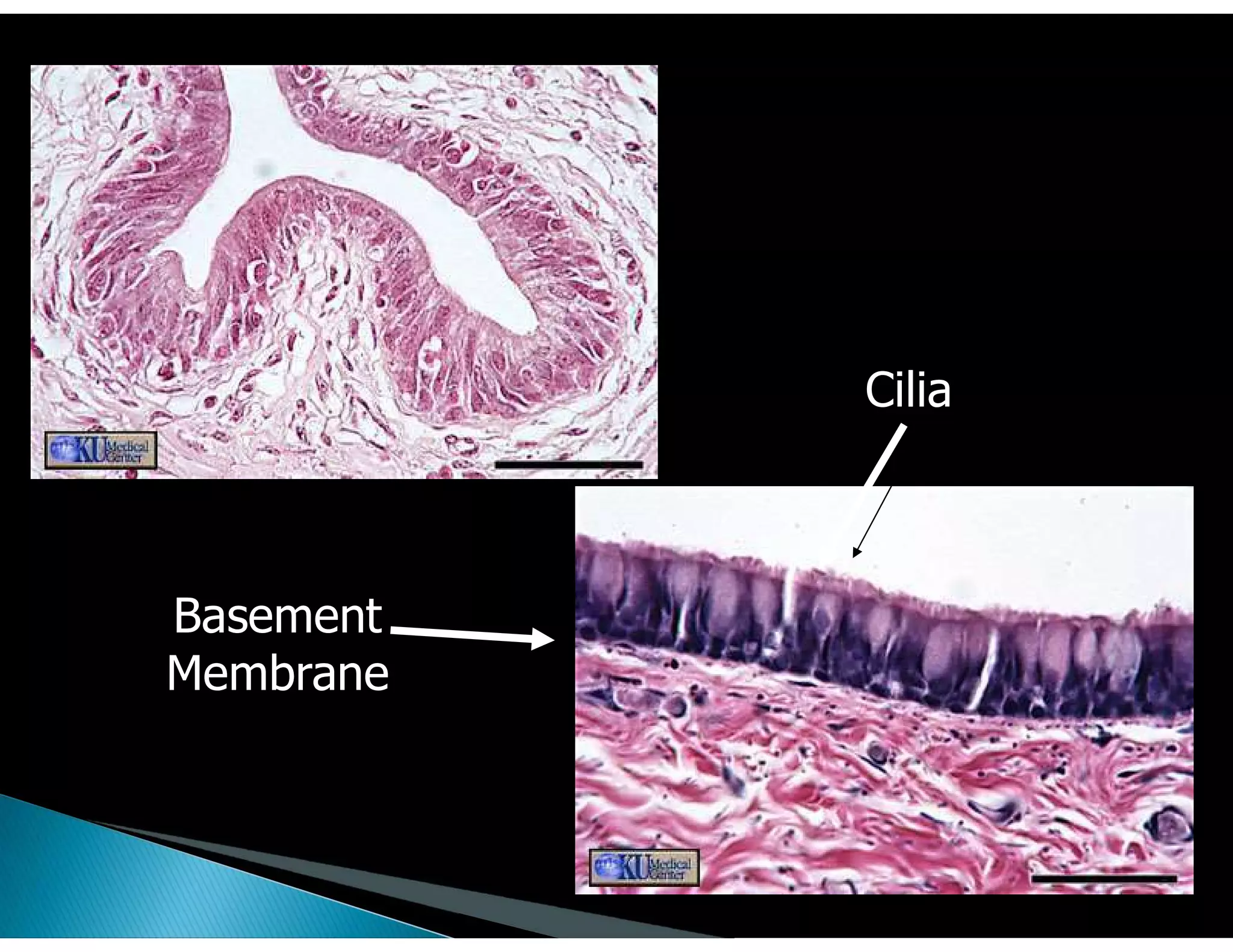
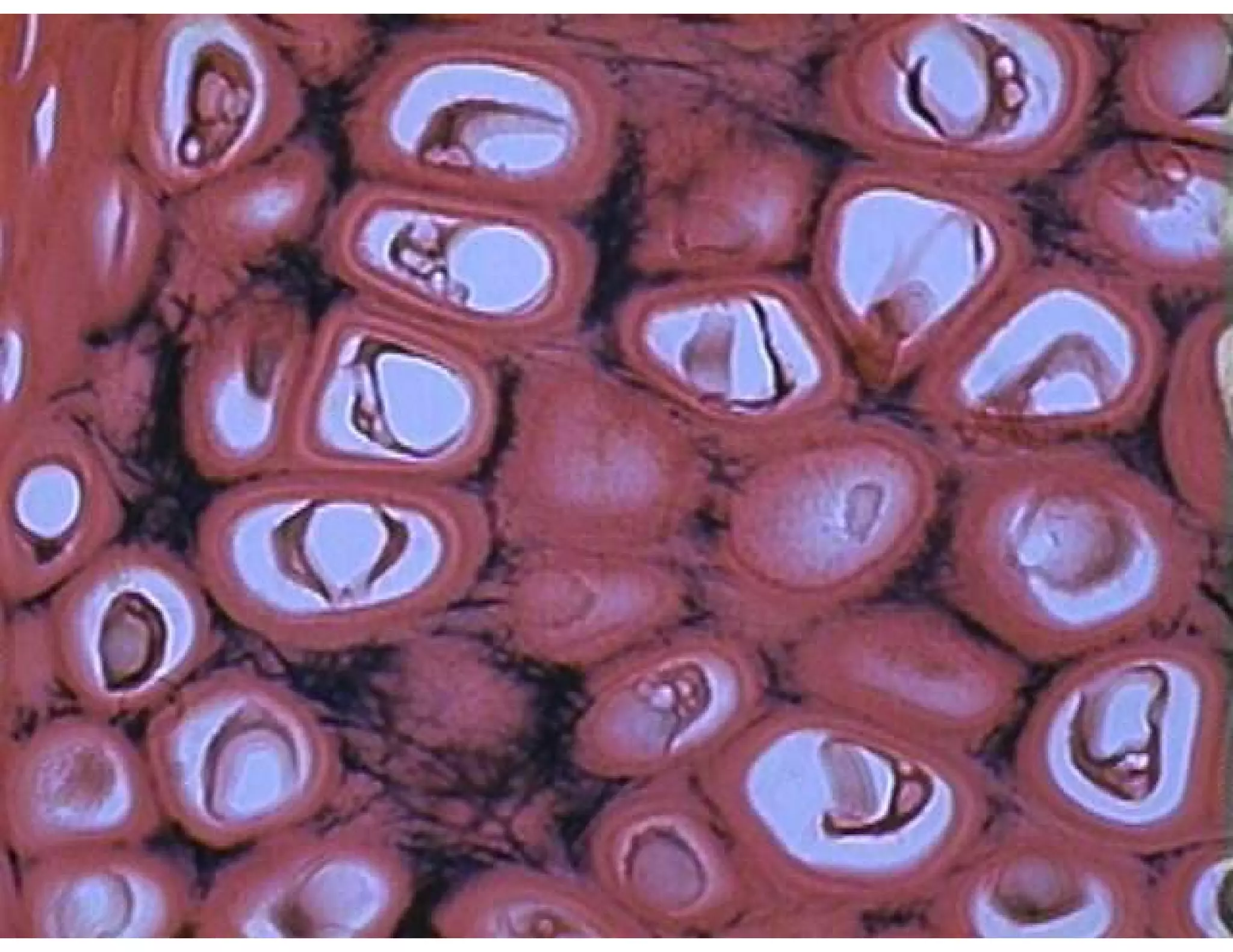
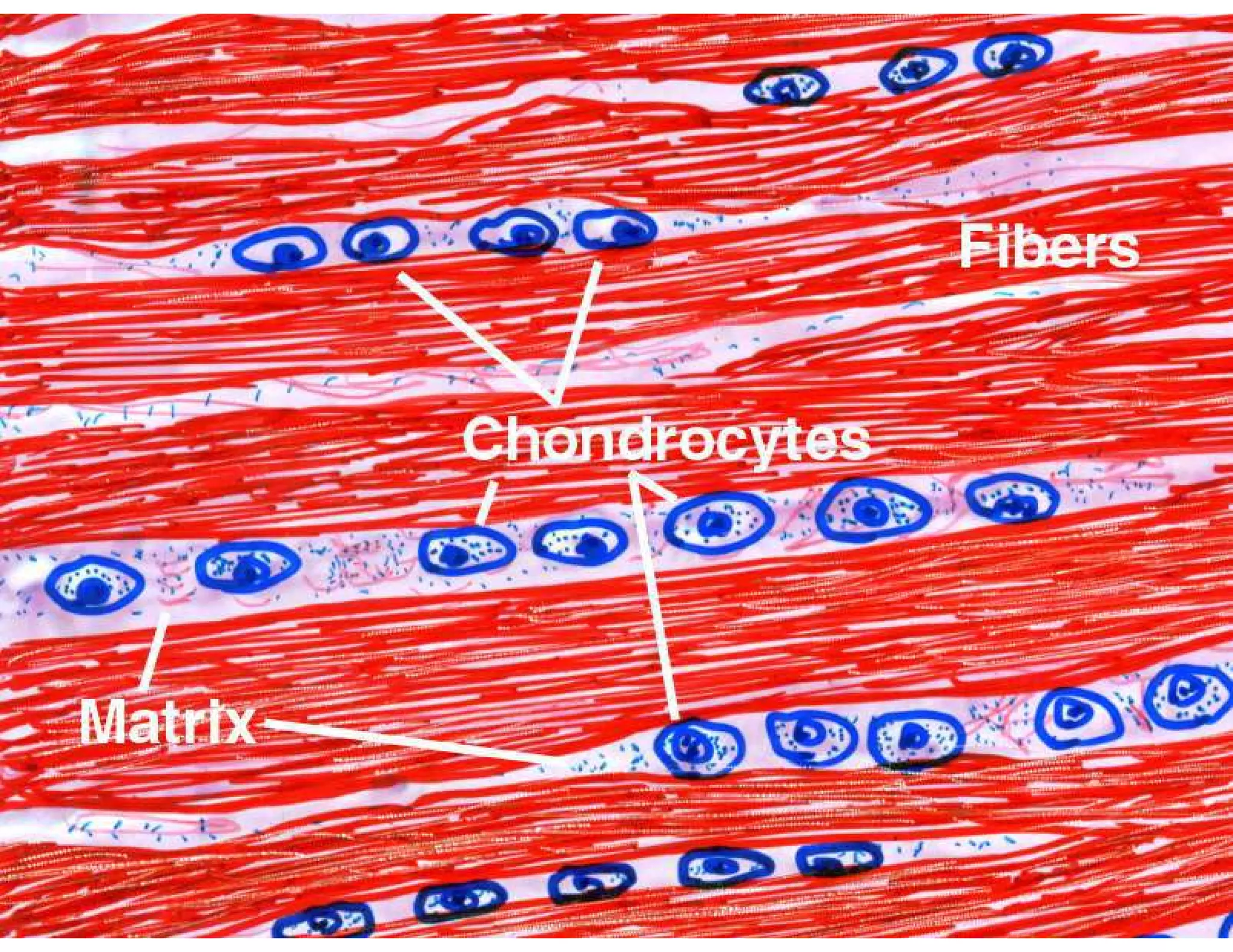
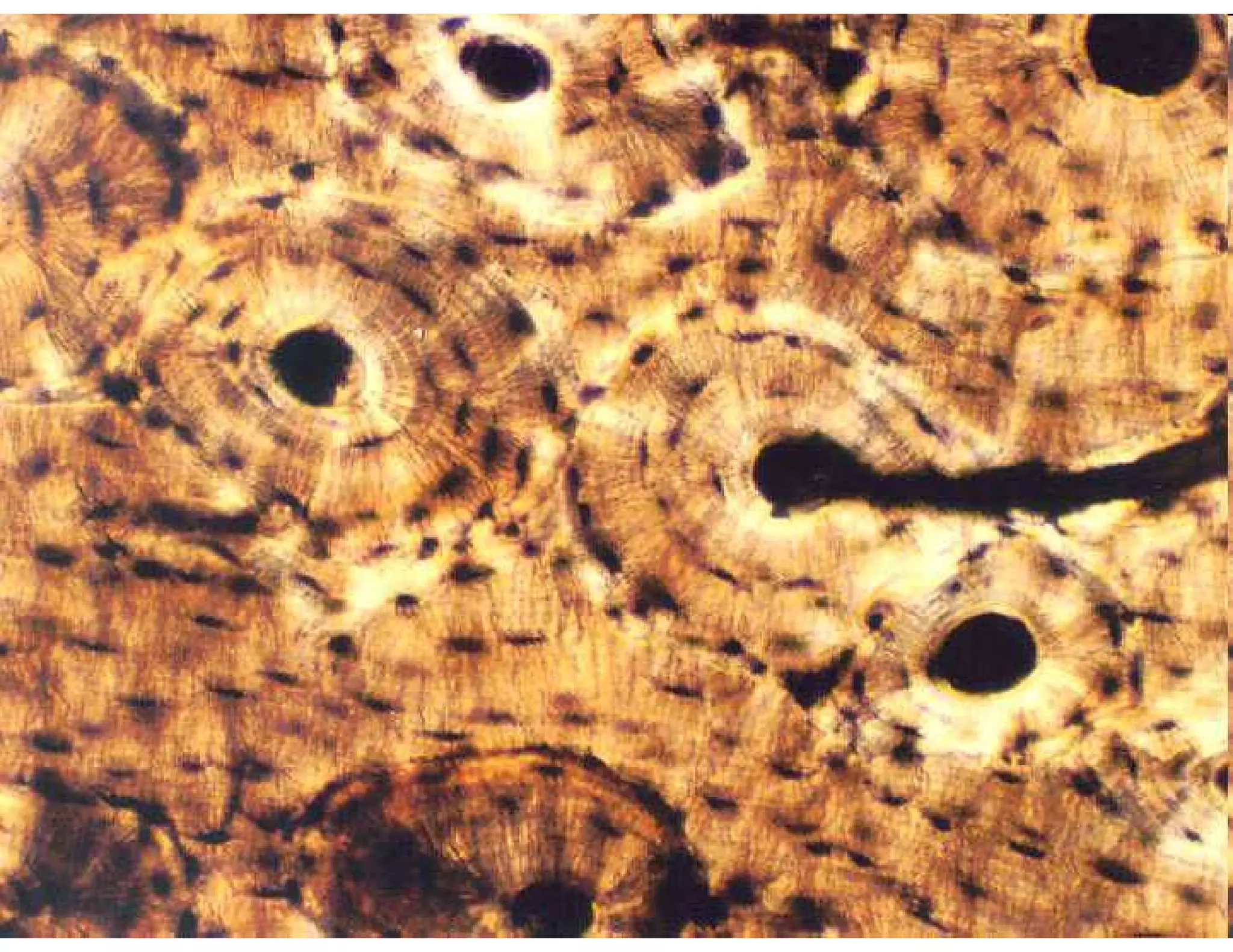
Focus on anatomical studies involving histology, embryology, and the structure of various tissues.
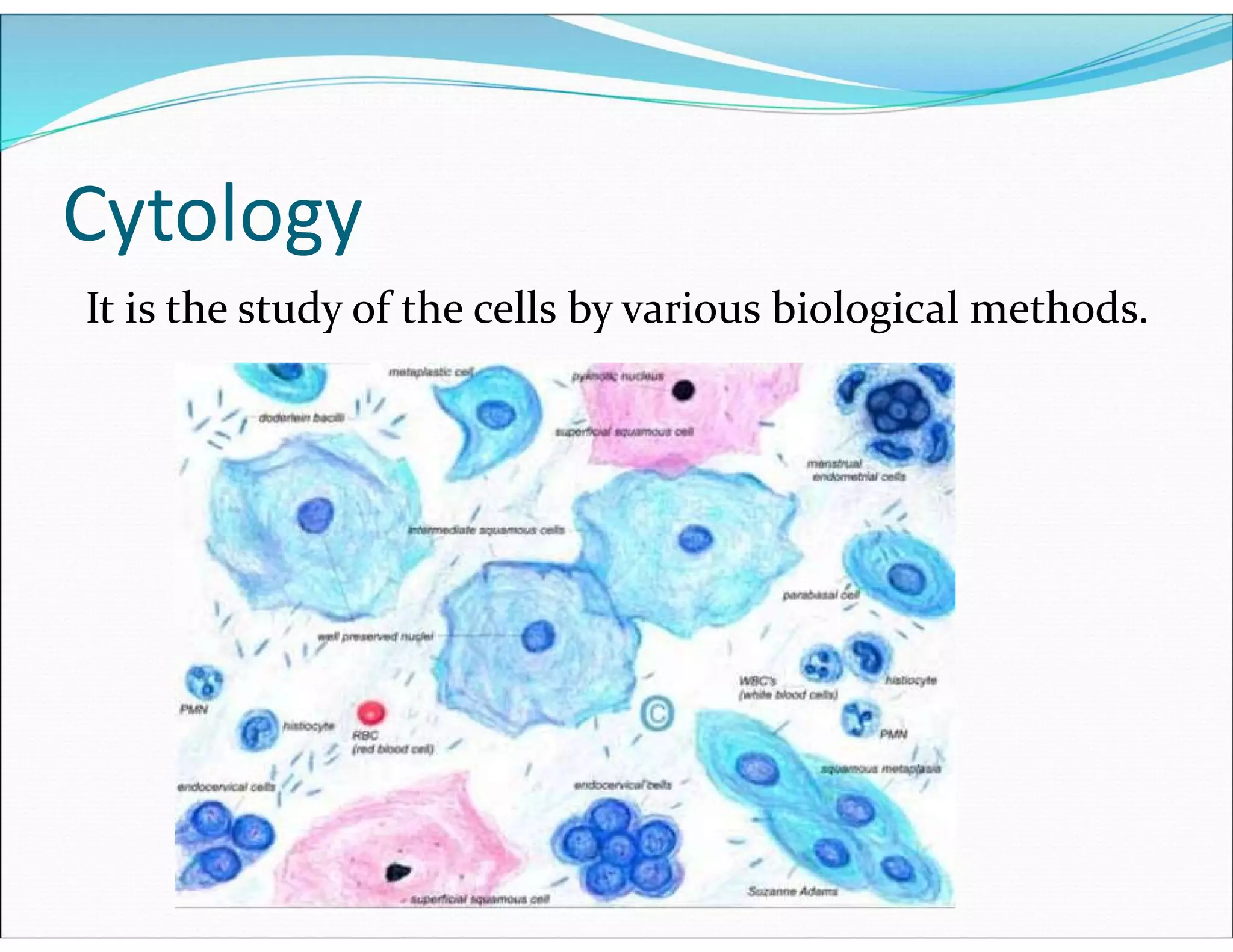
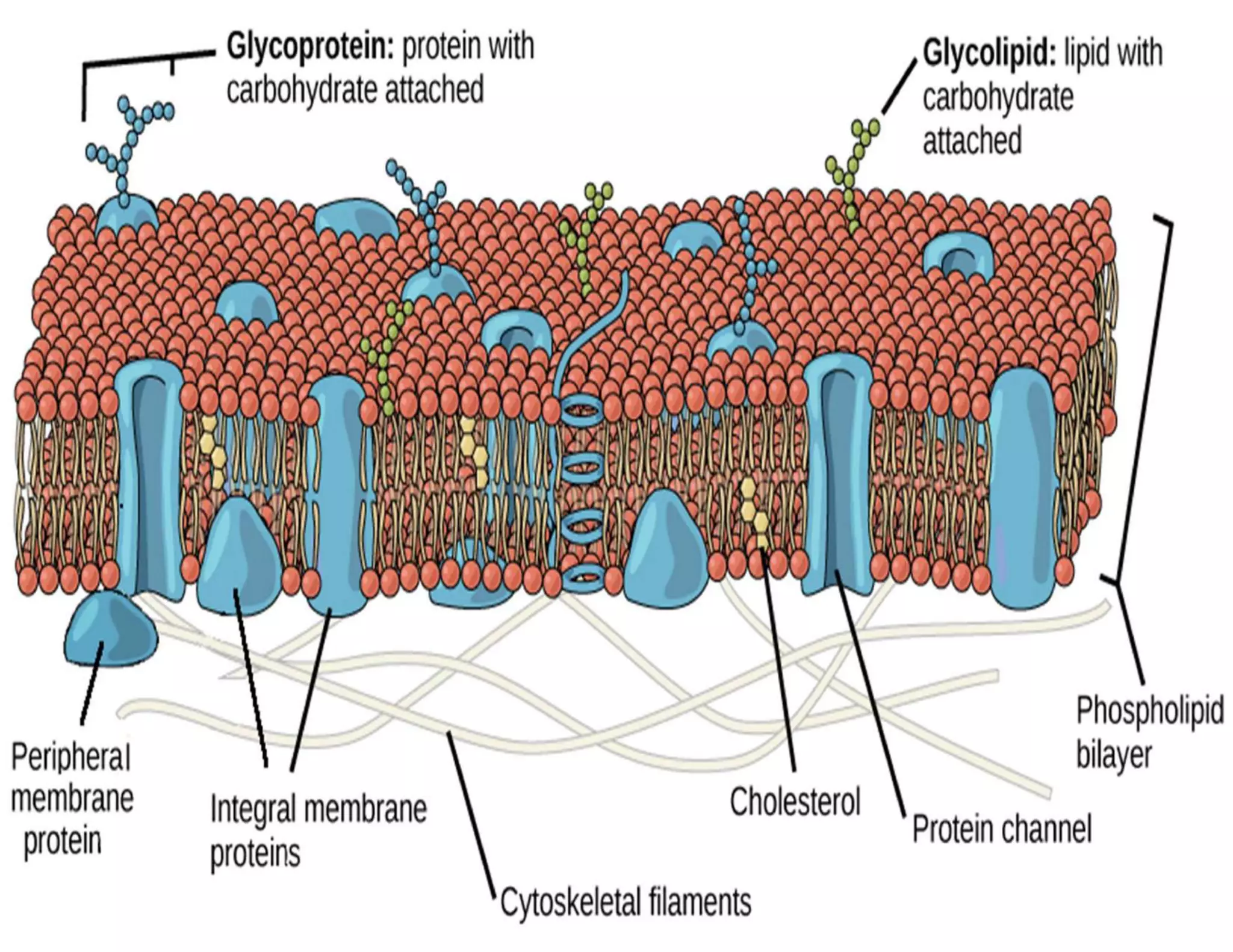
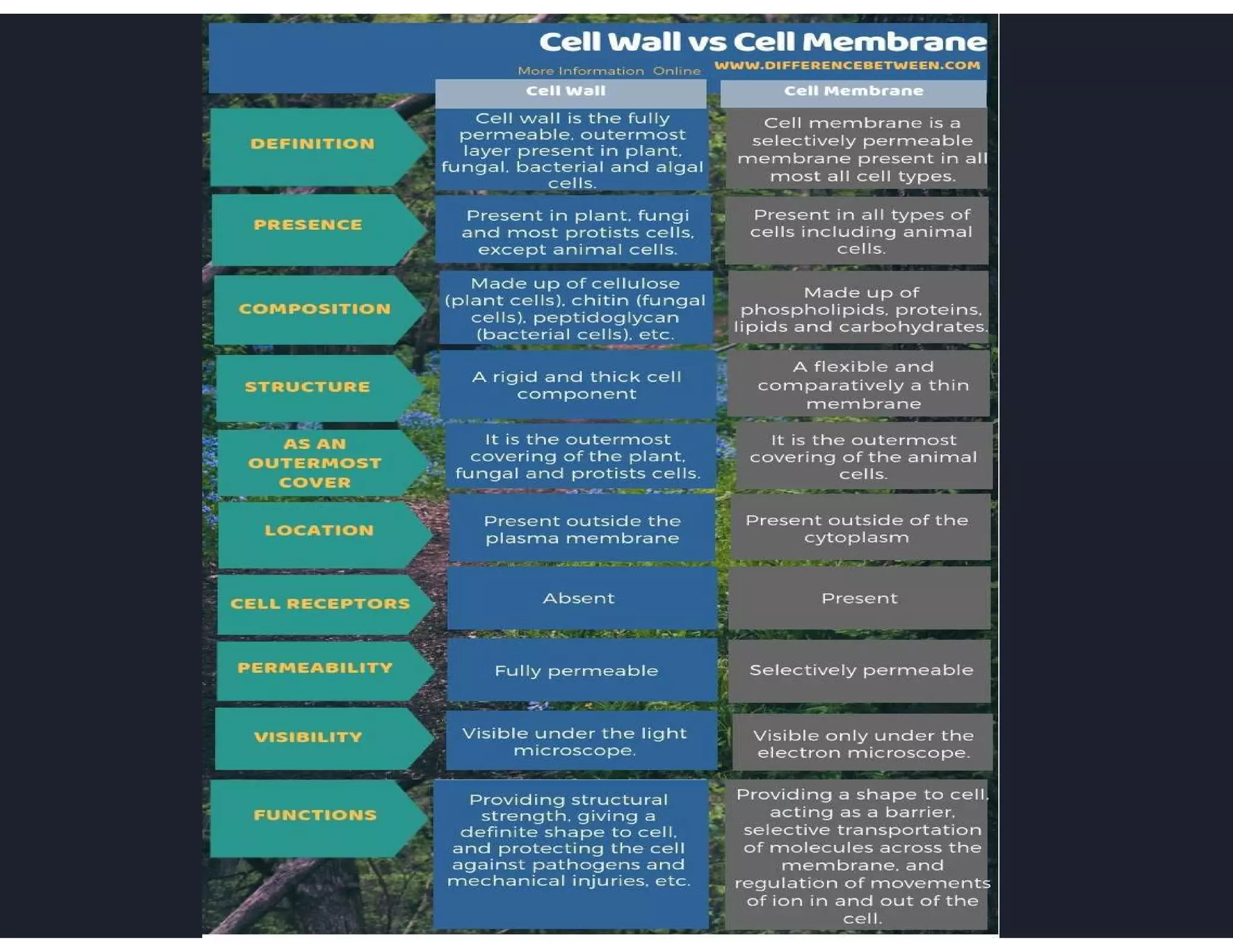
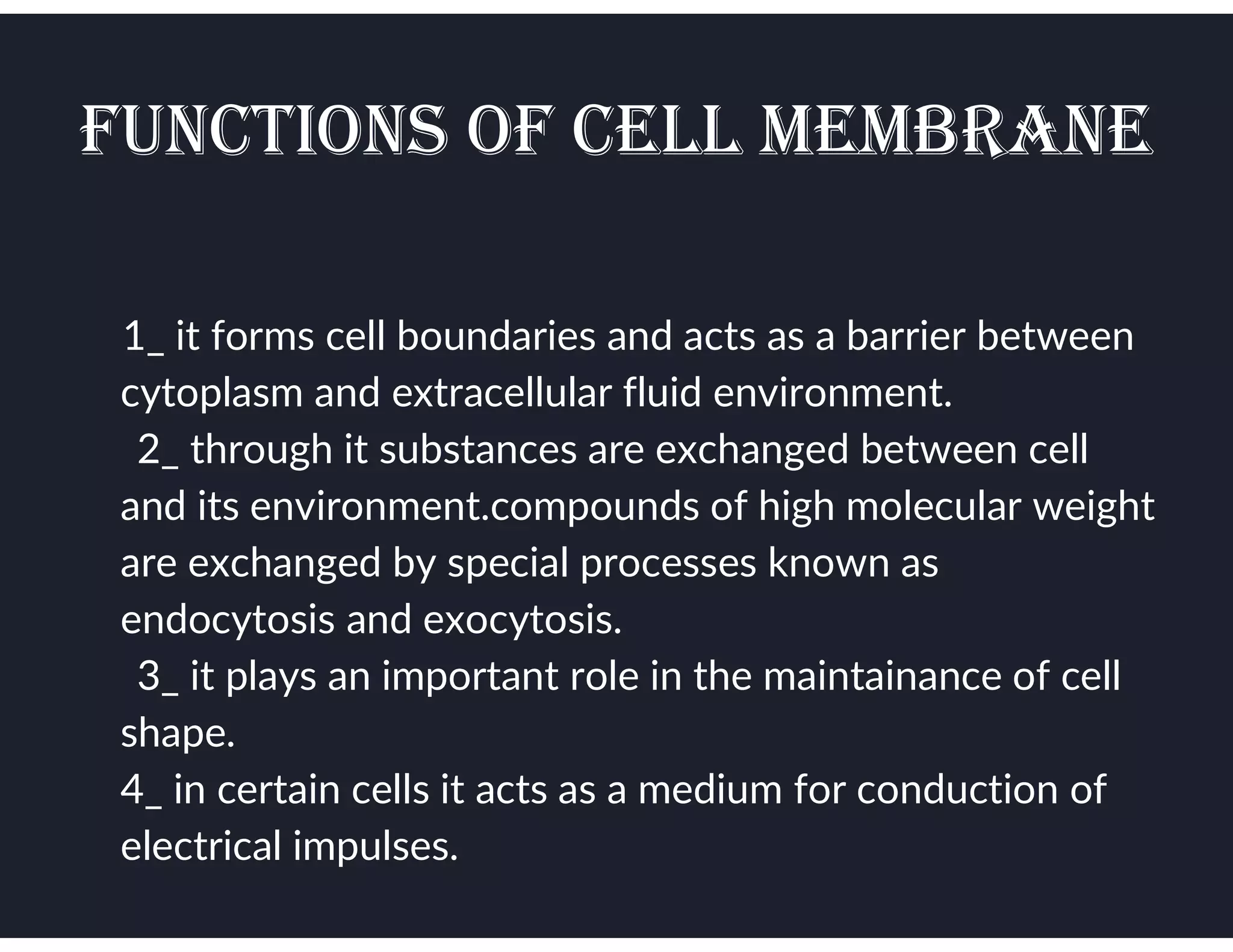
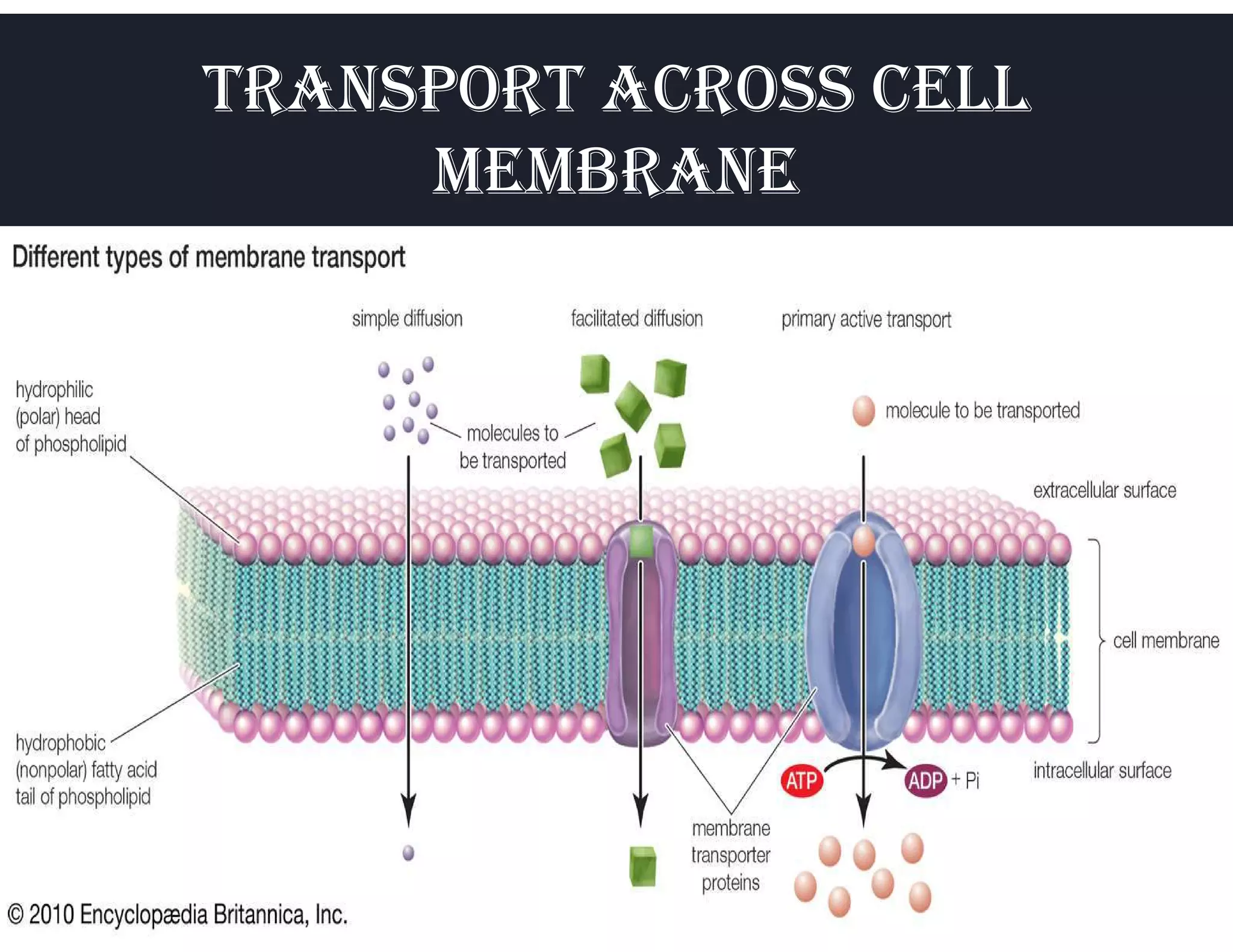
Detailed overview of cell structures, functions, and cellular organization.
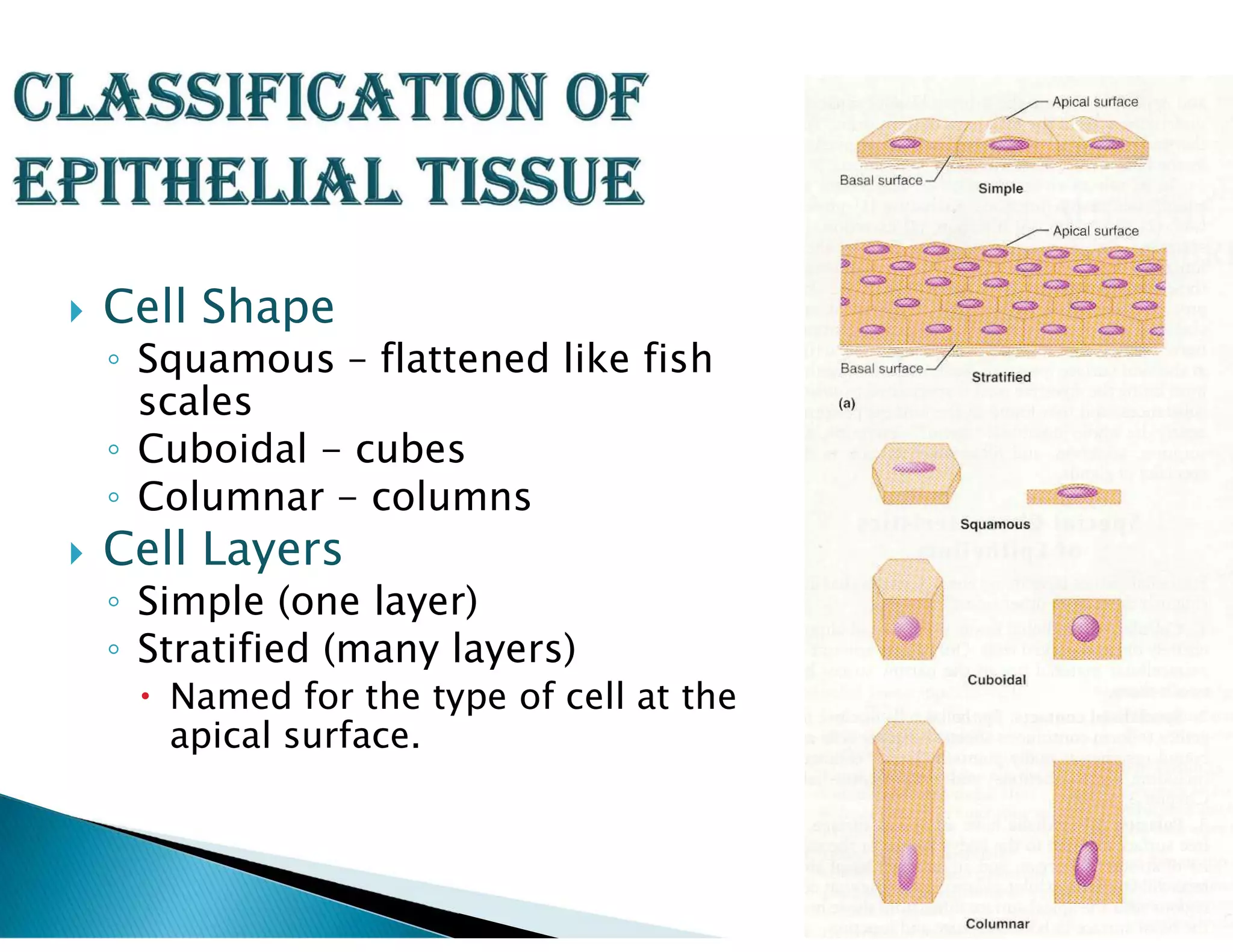
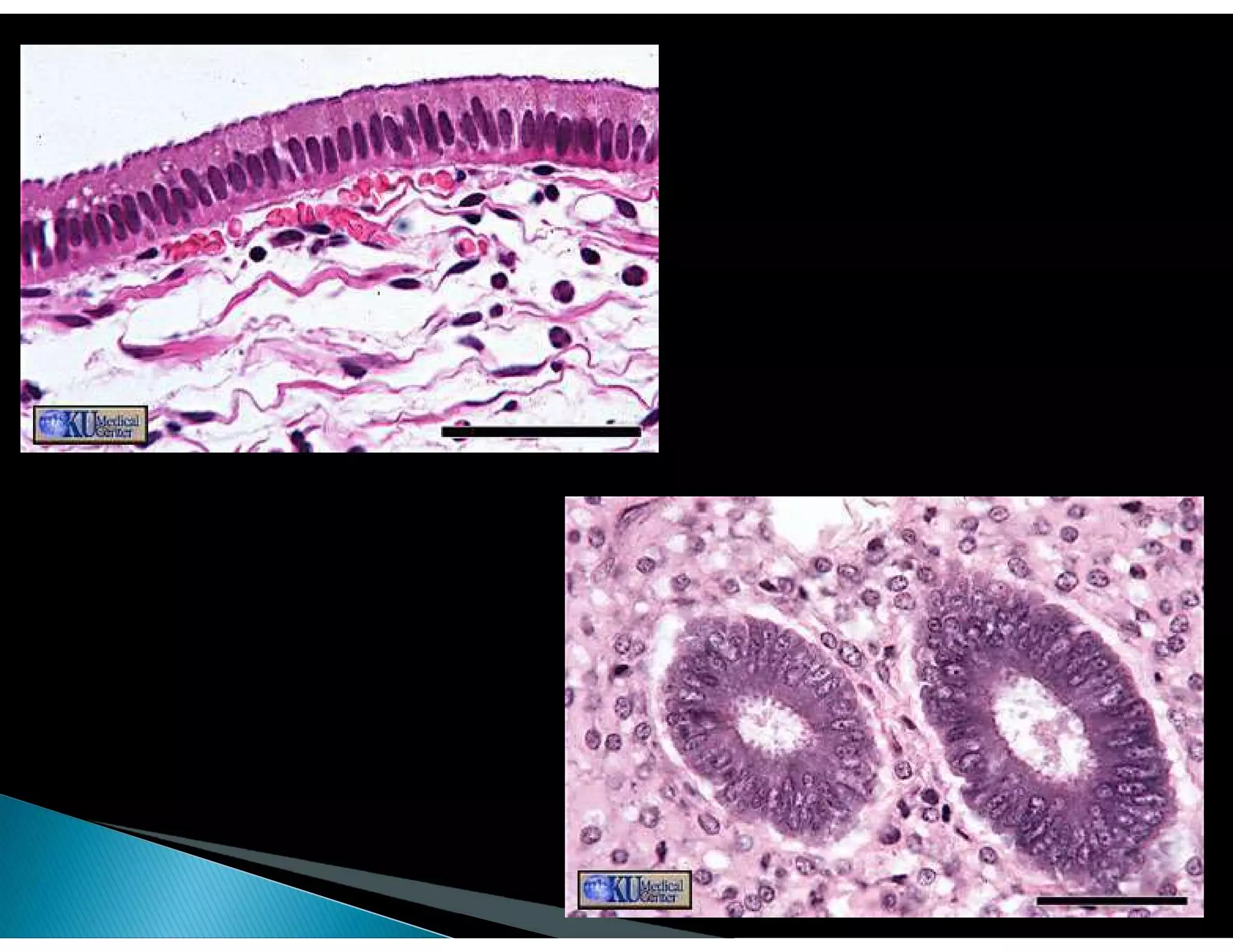
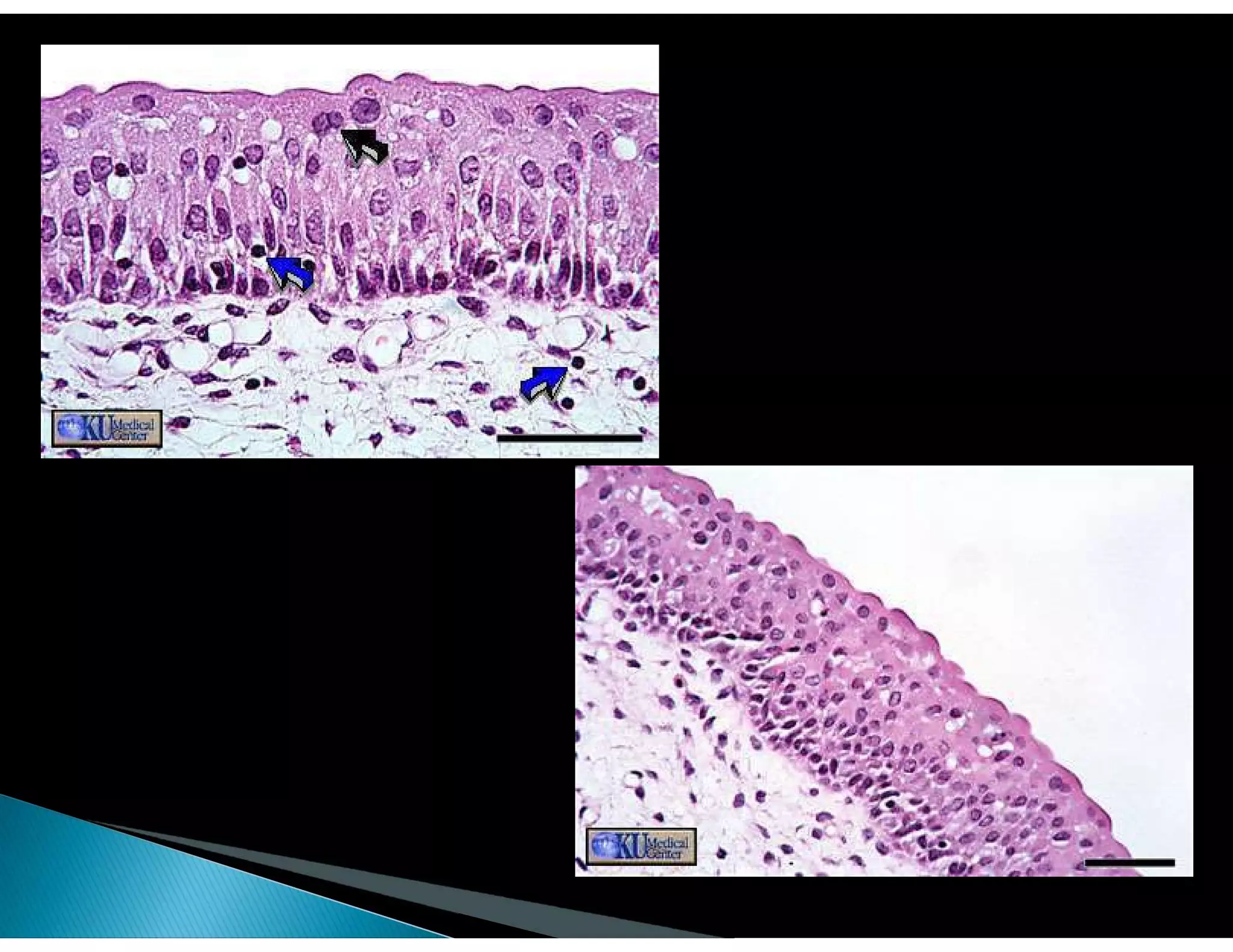
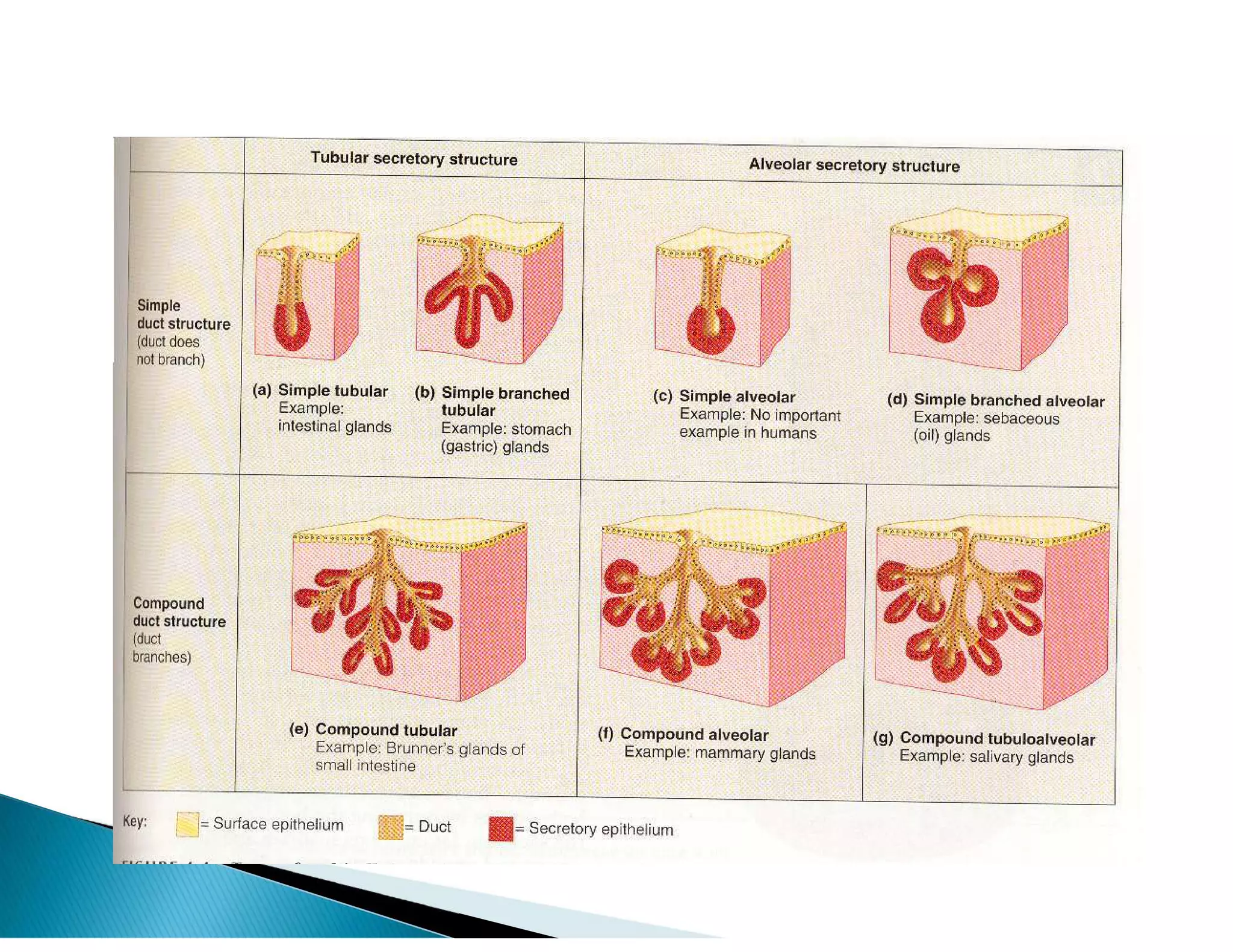
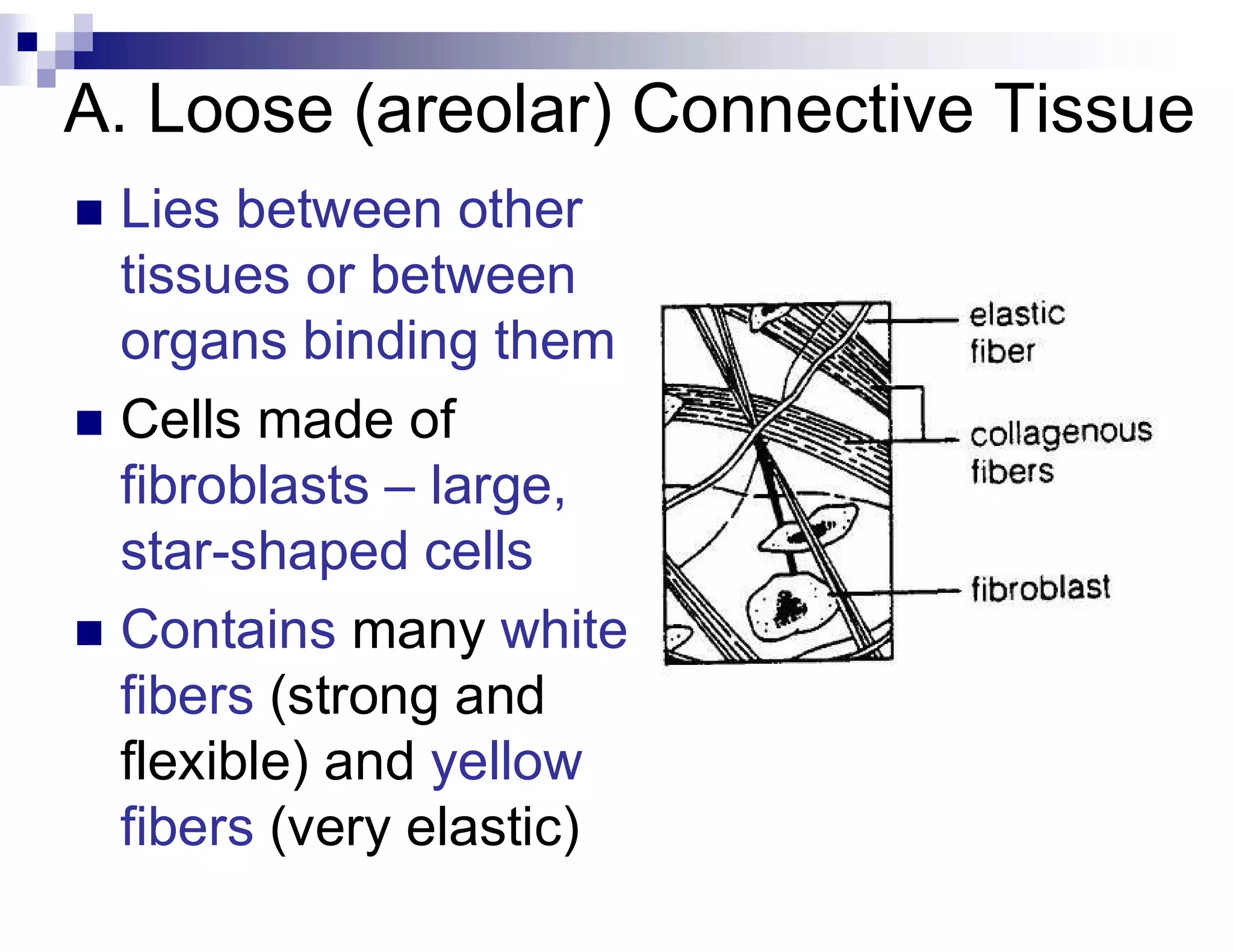
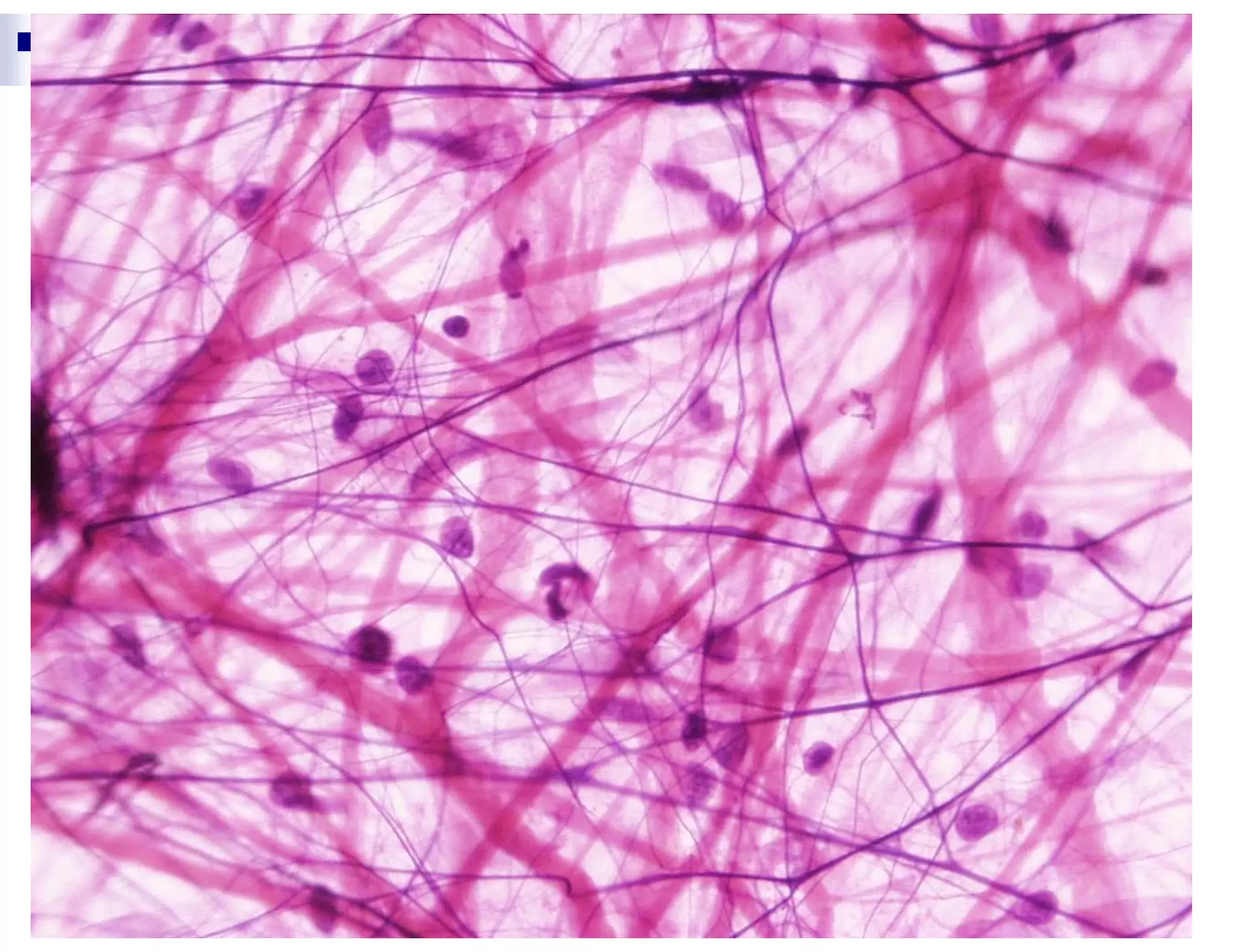
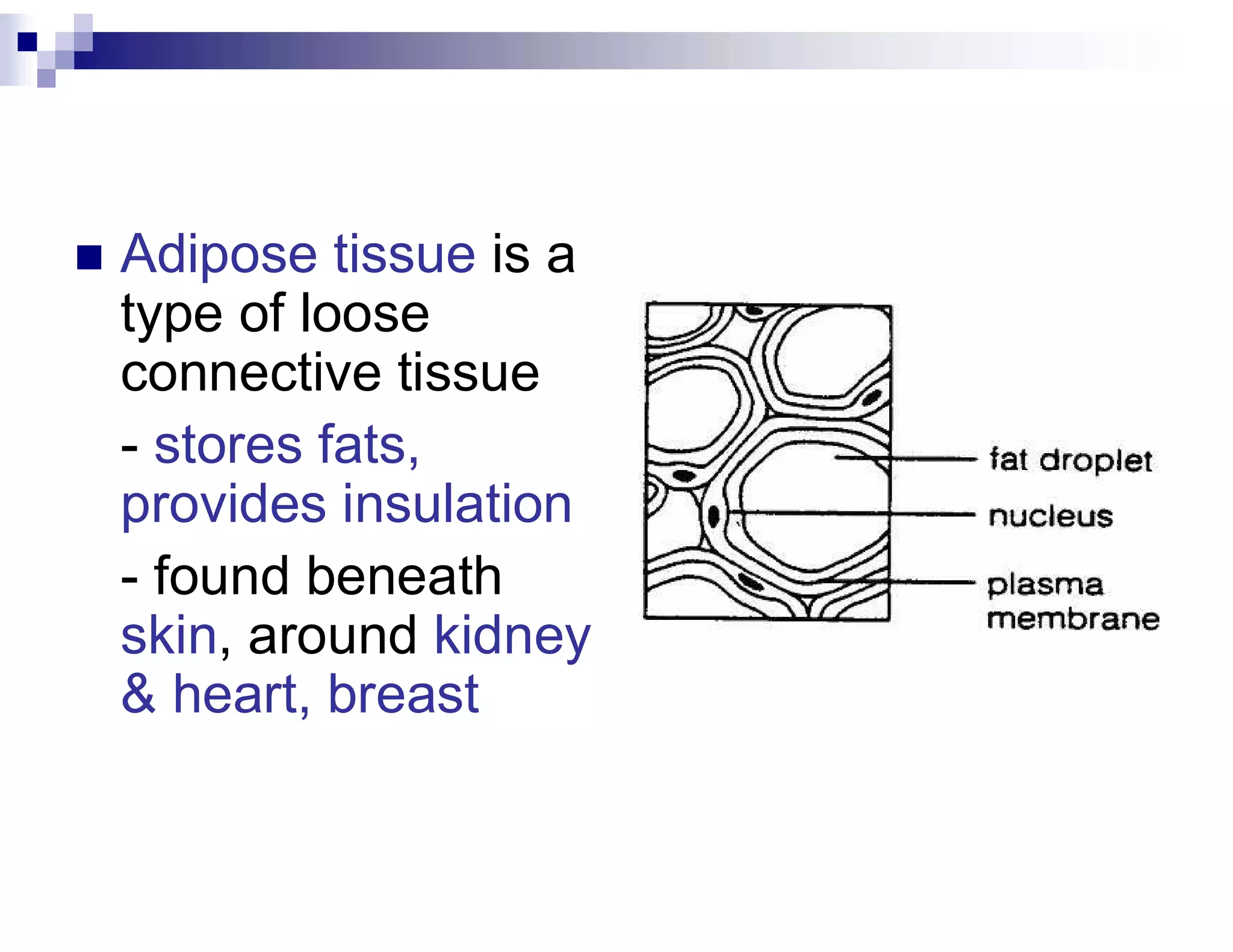
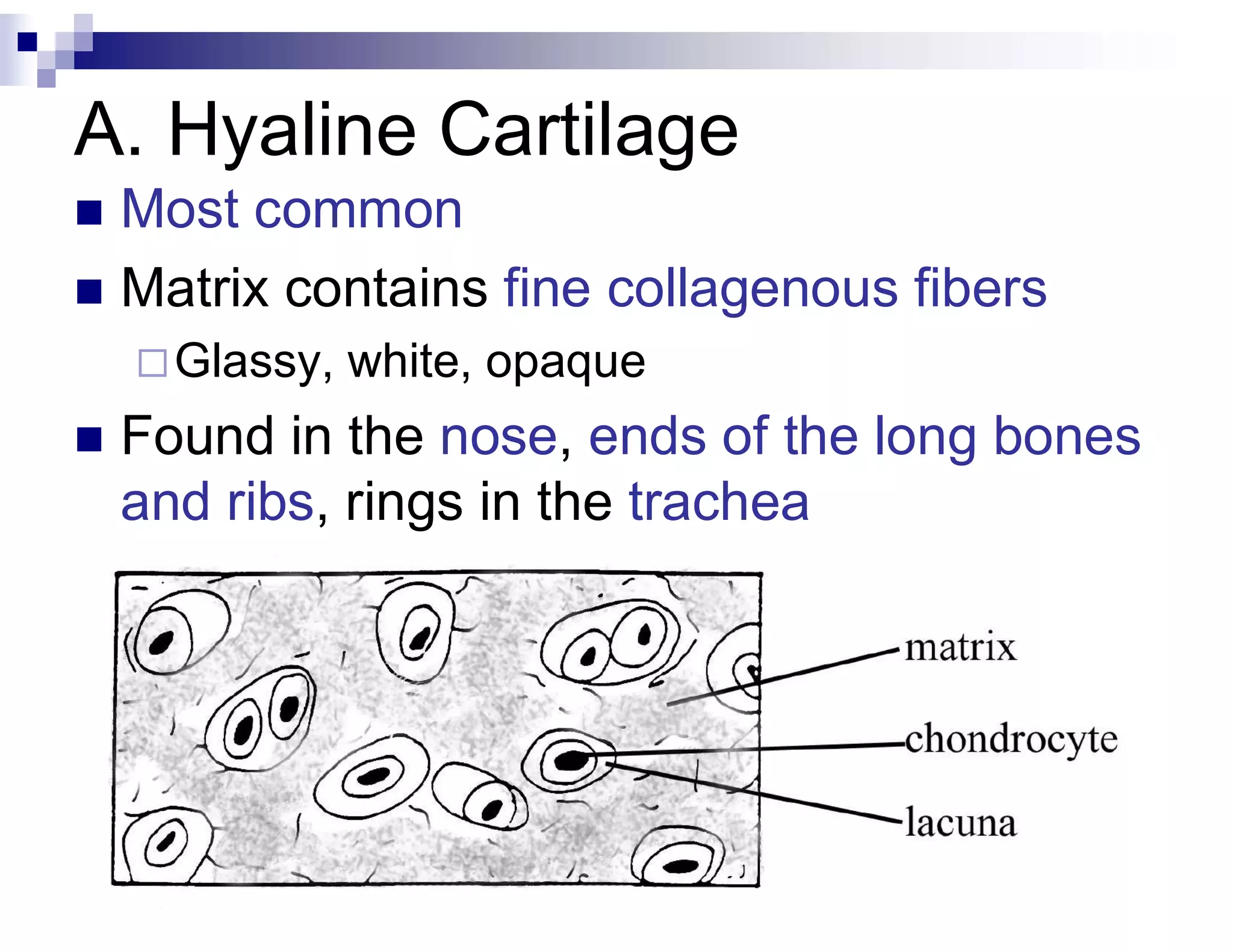
Description of various tissue types, their functions, and structural characteristics within human anatomy.
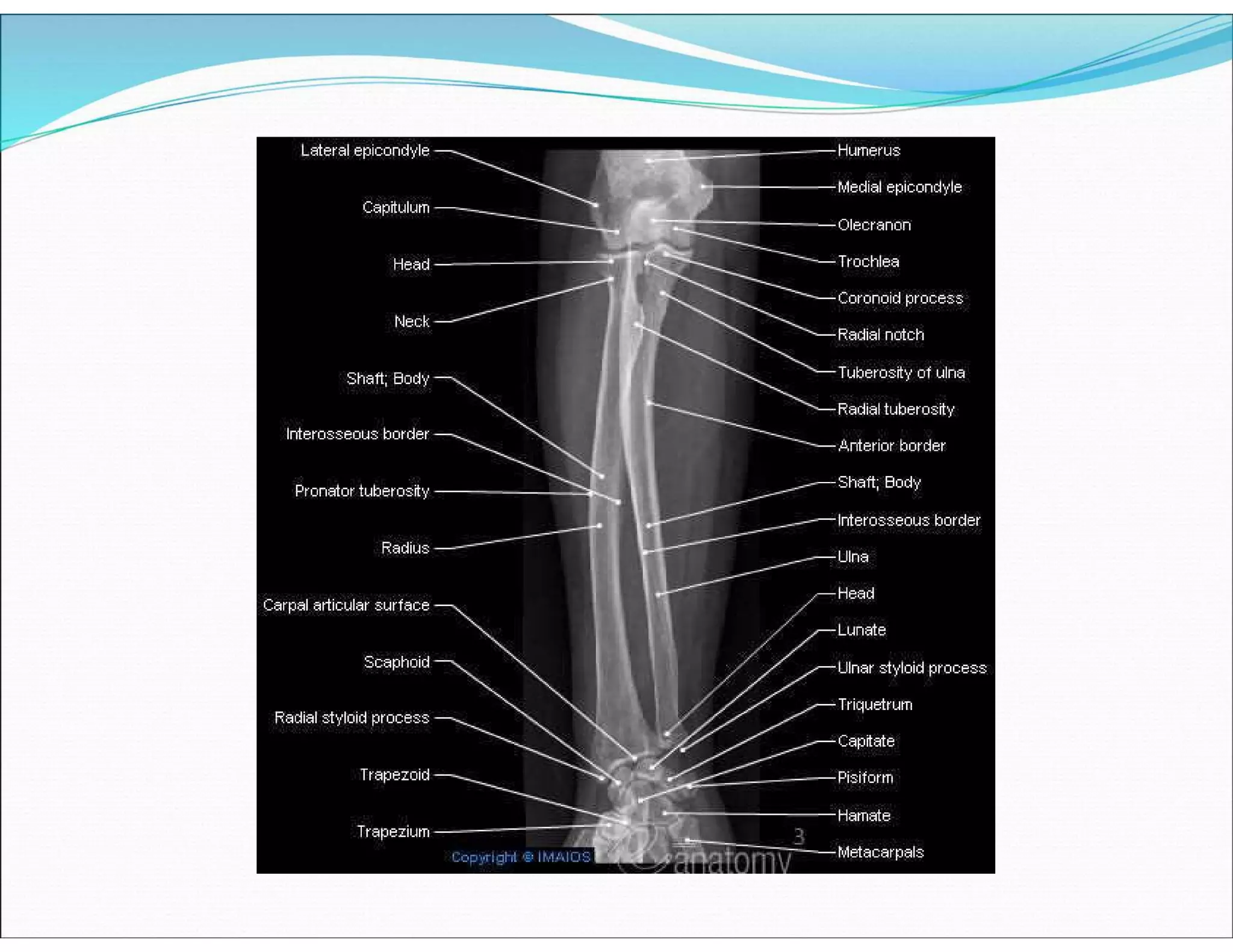
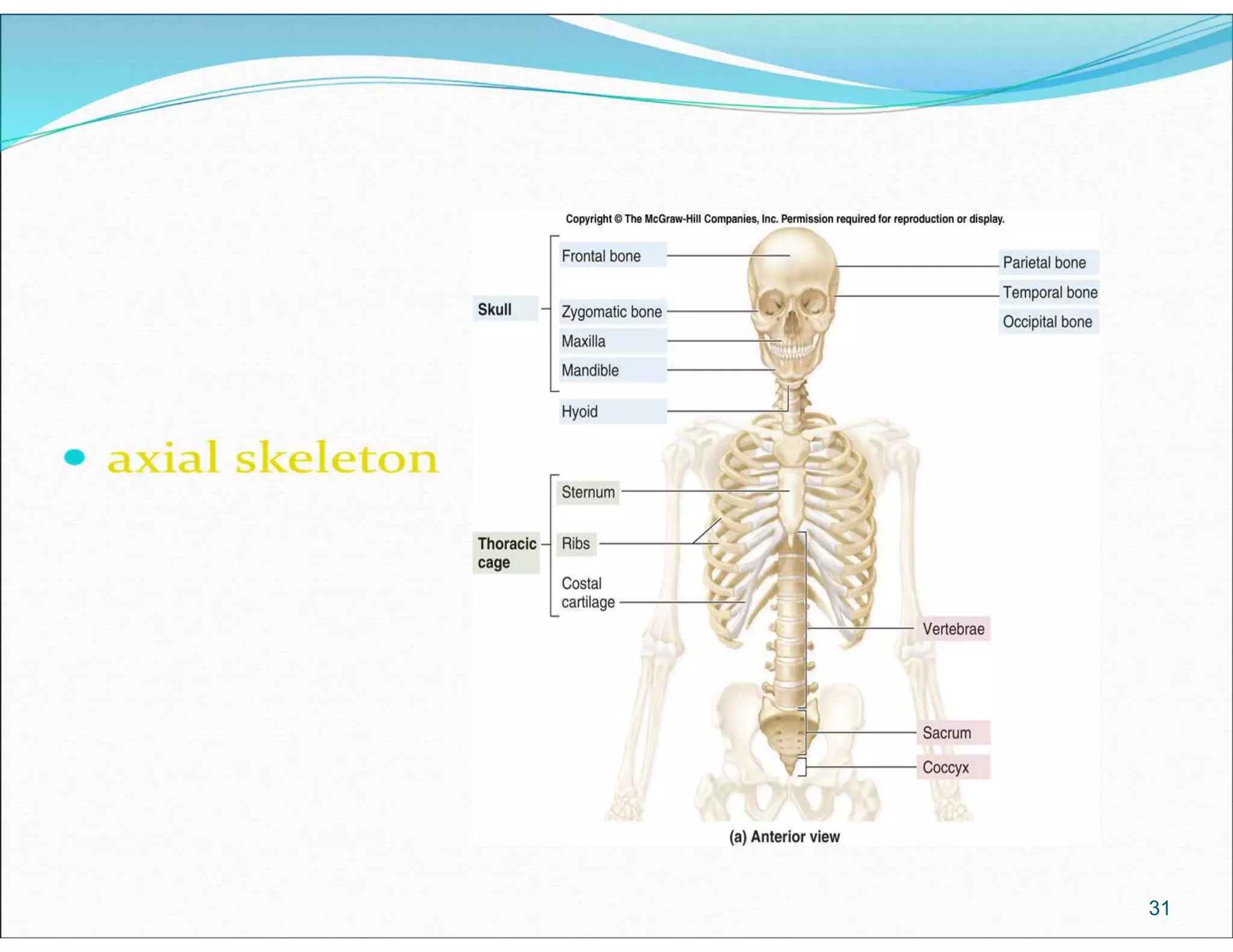
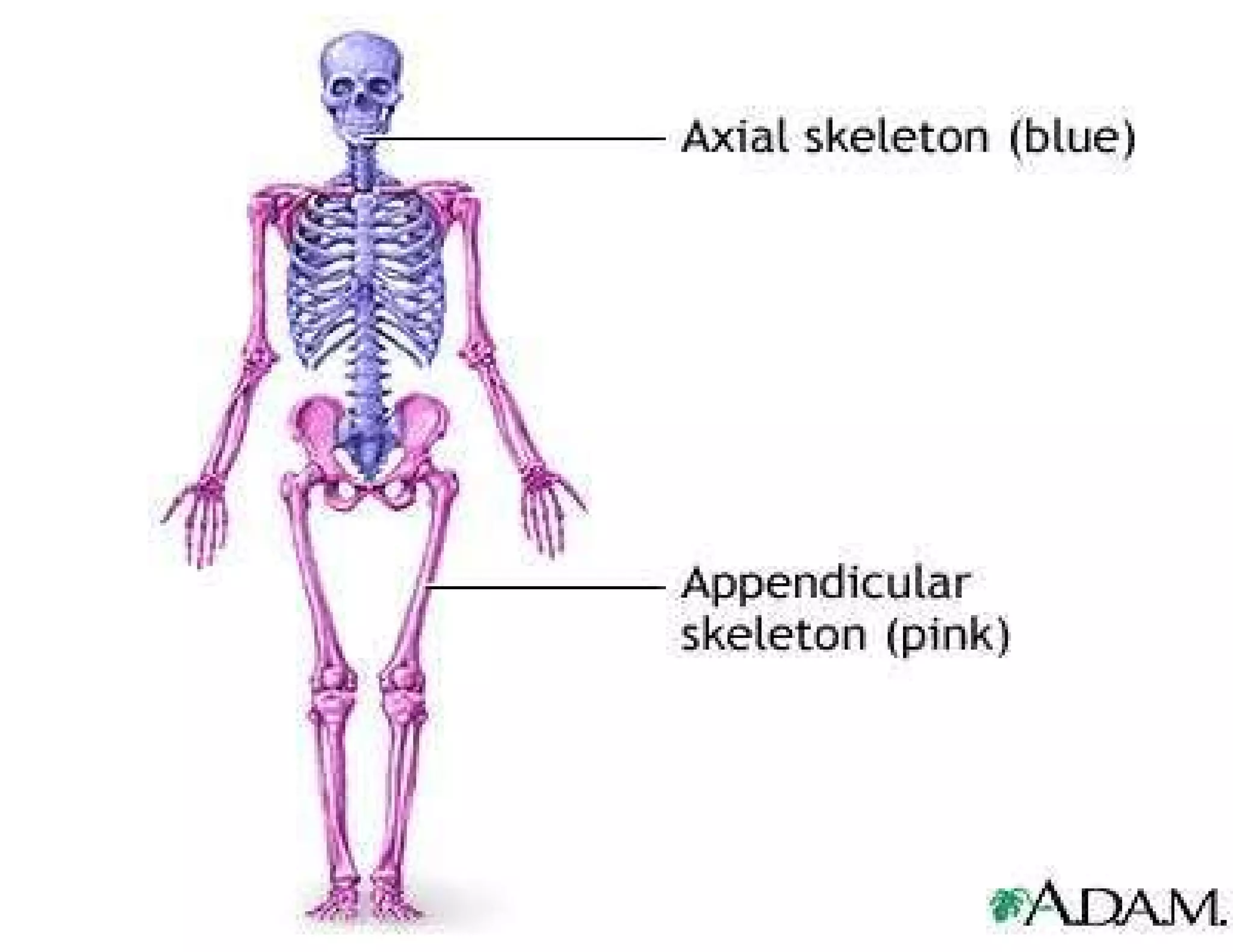
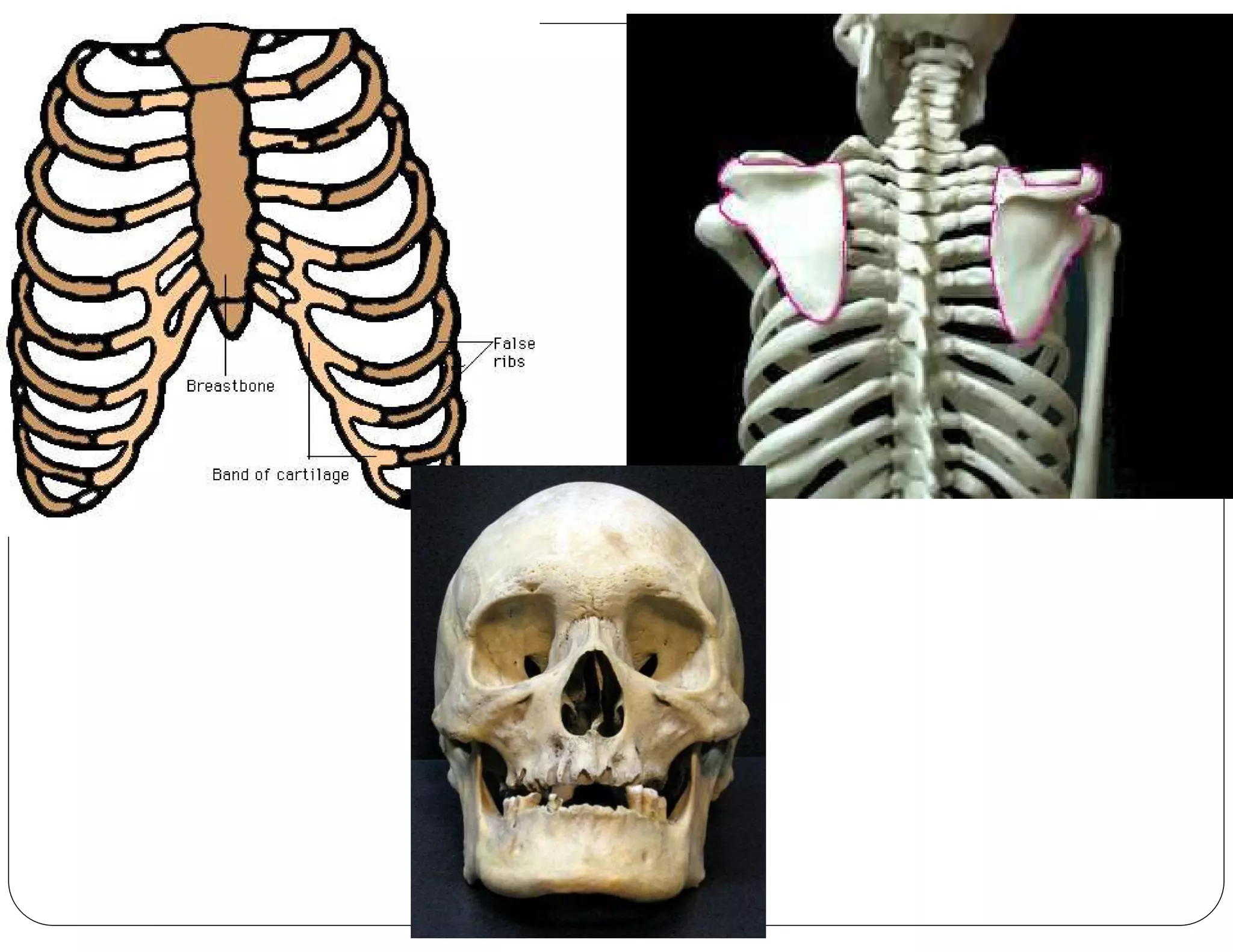
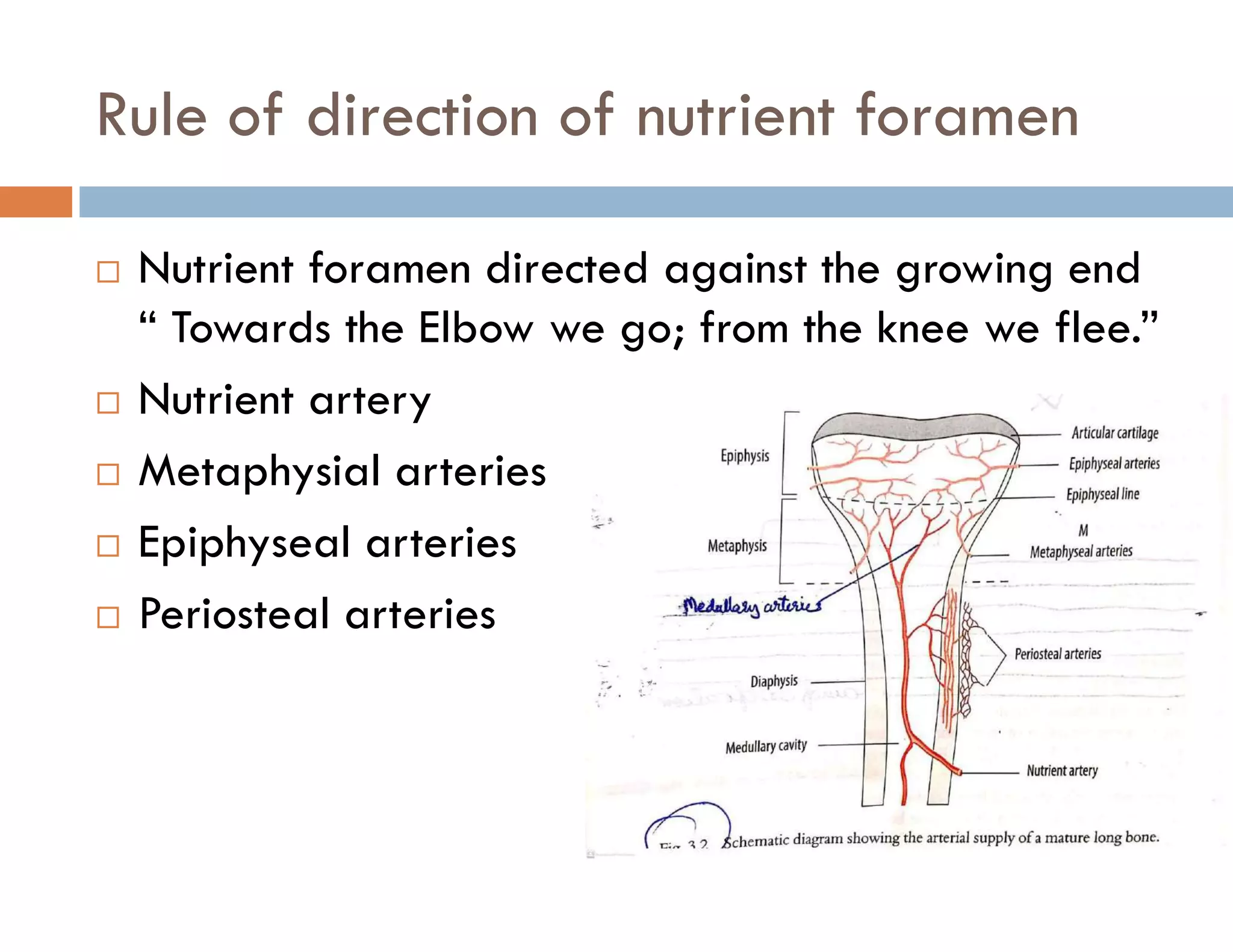
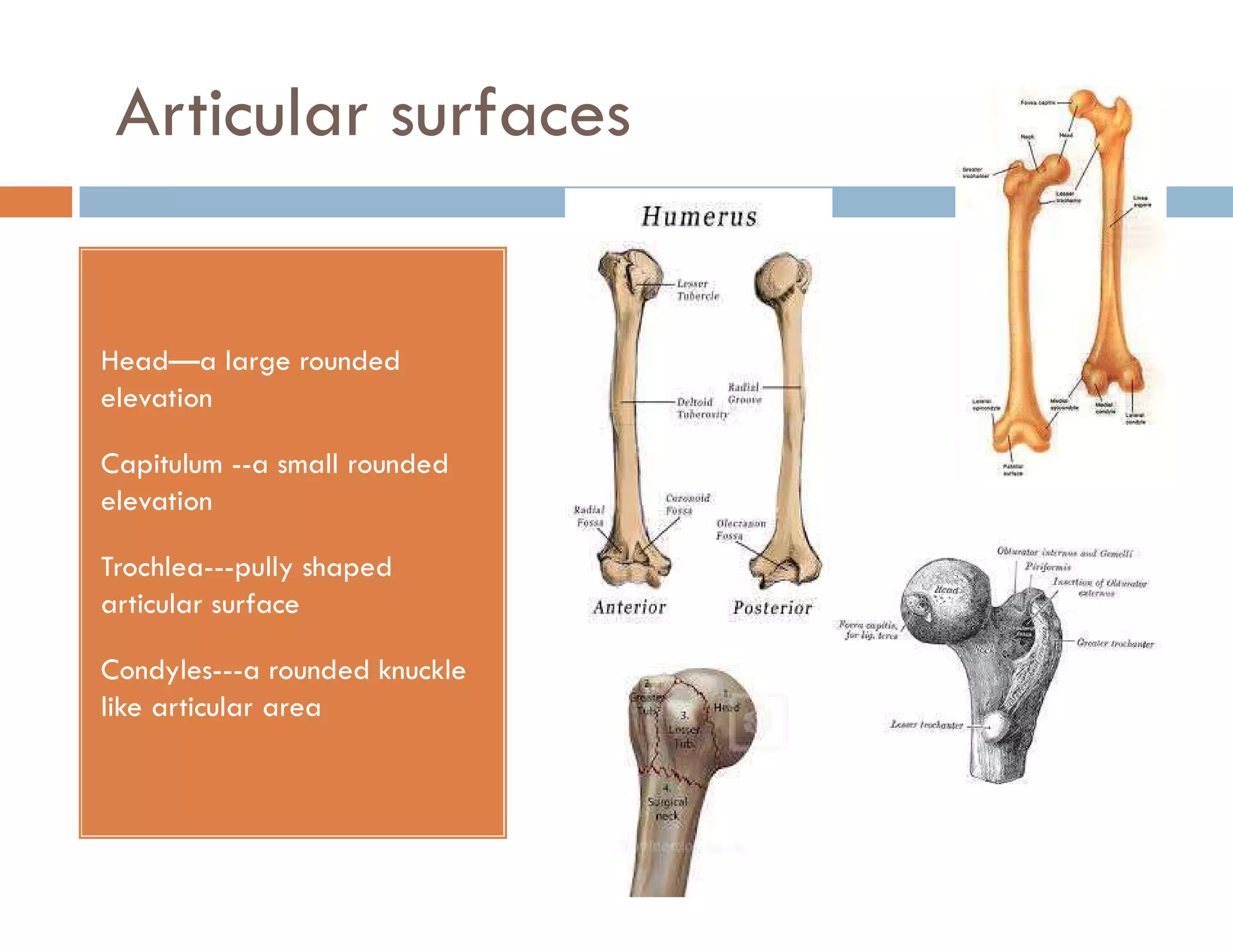
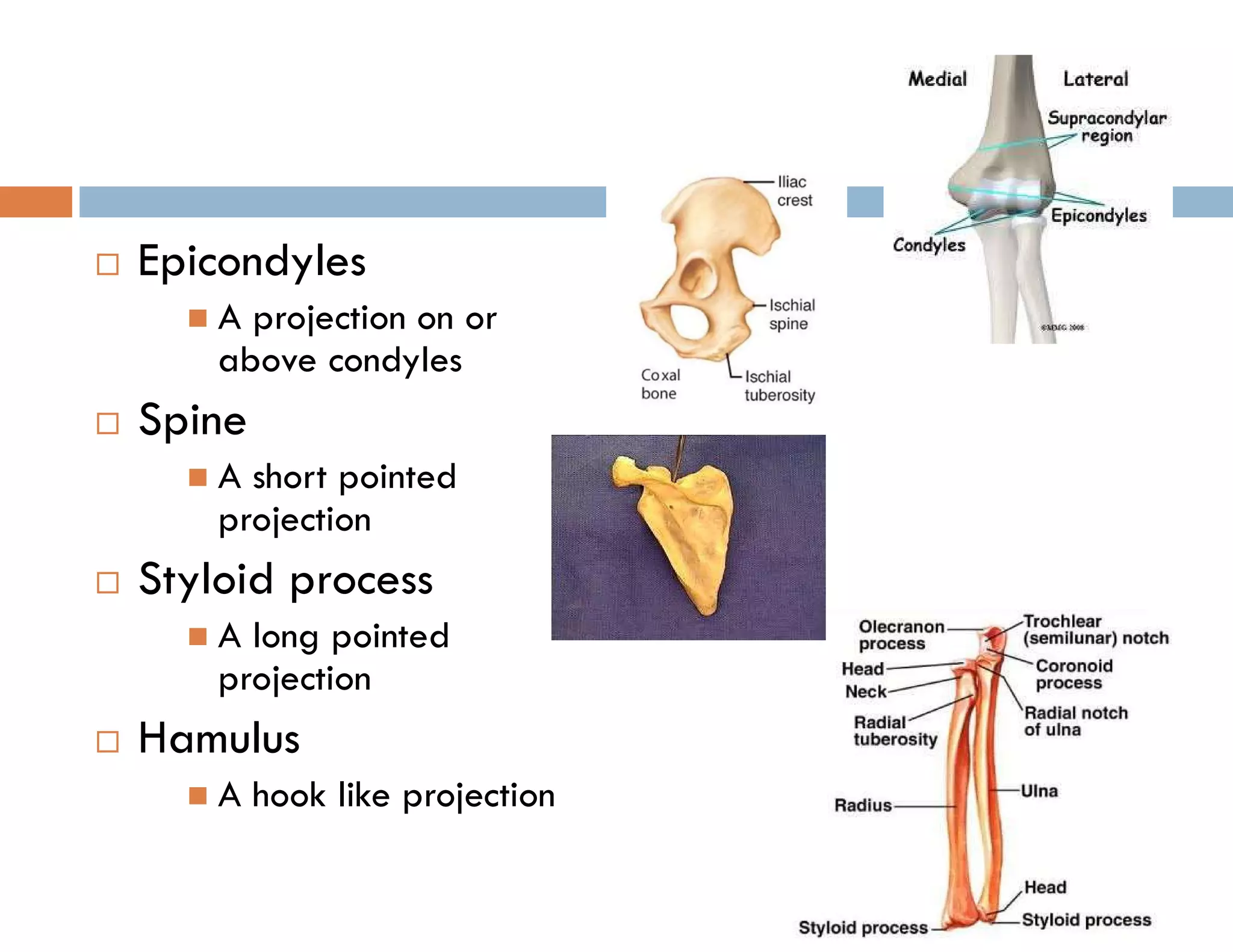
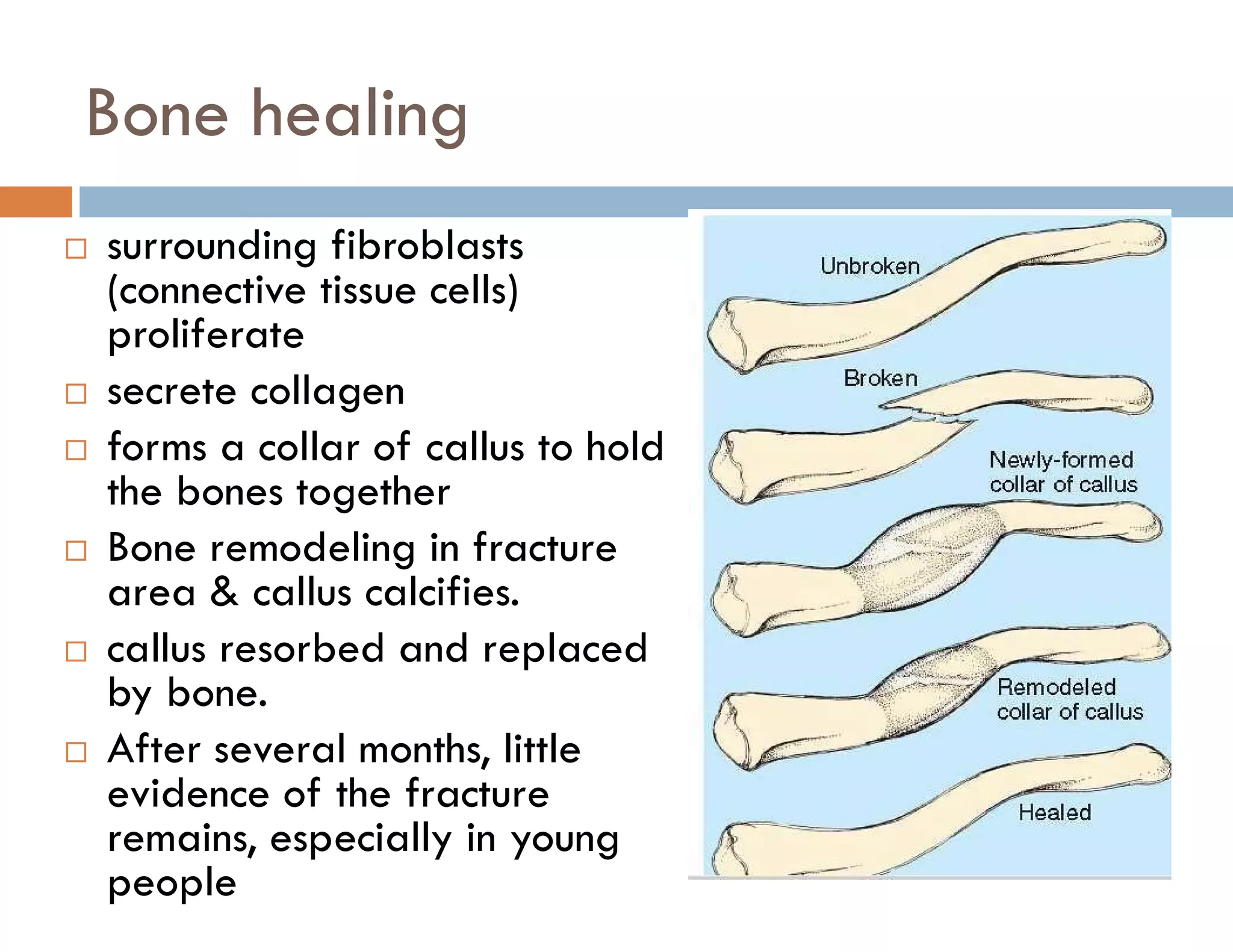
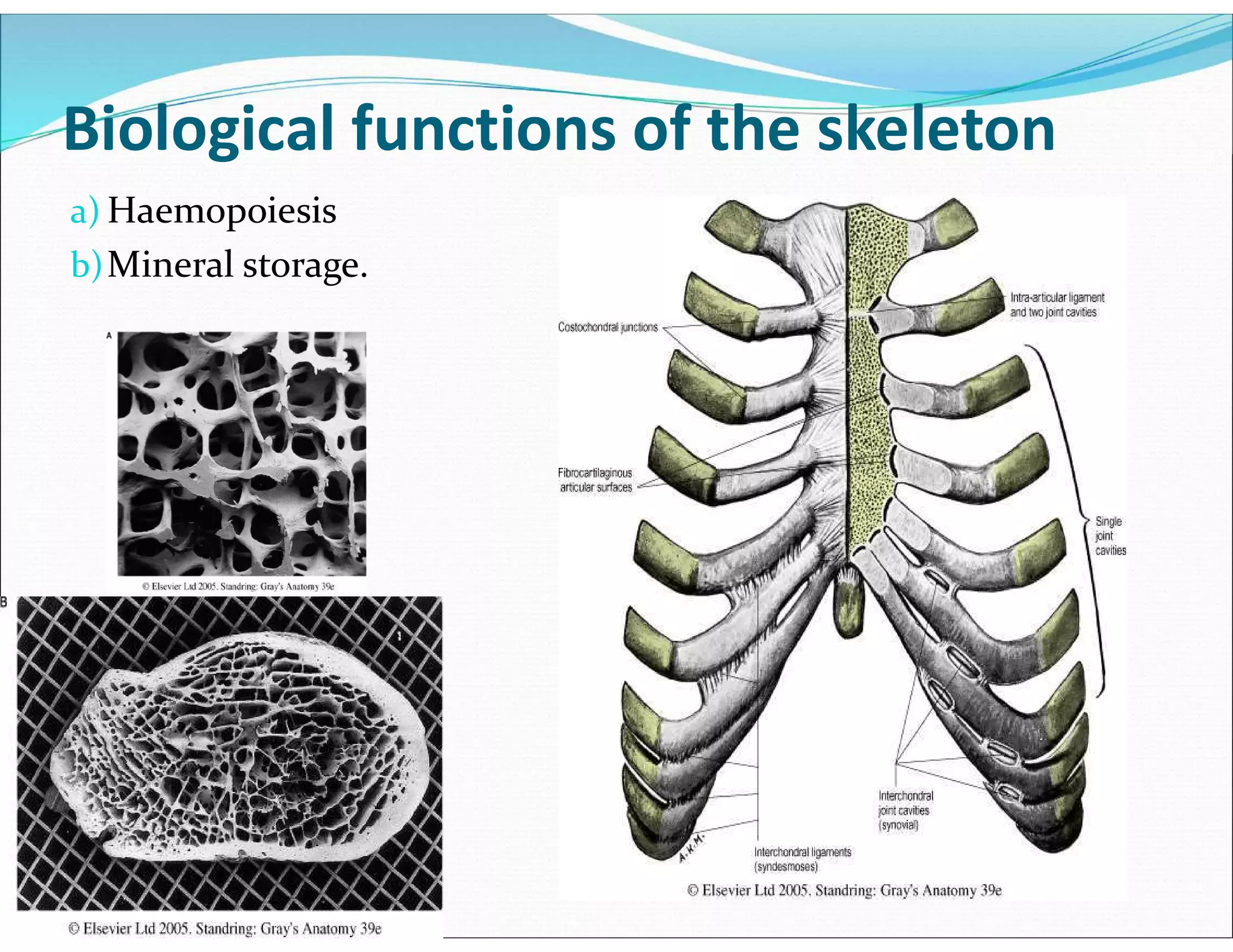
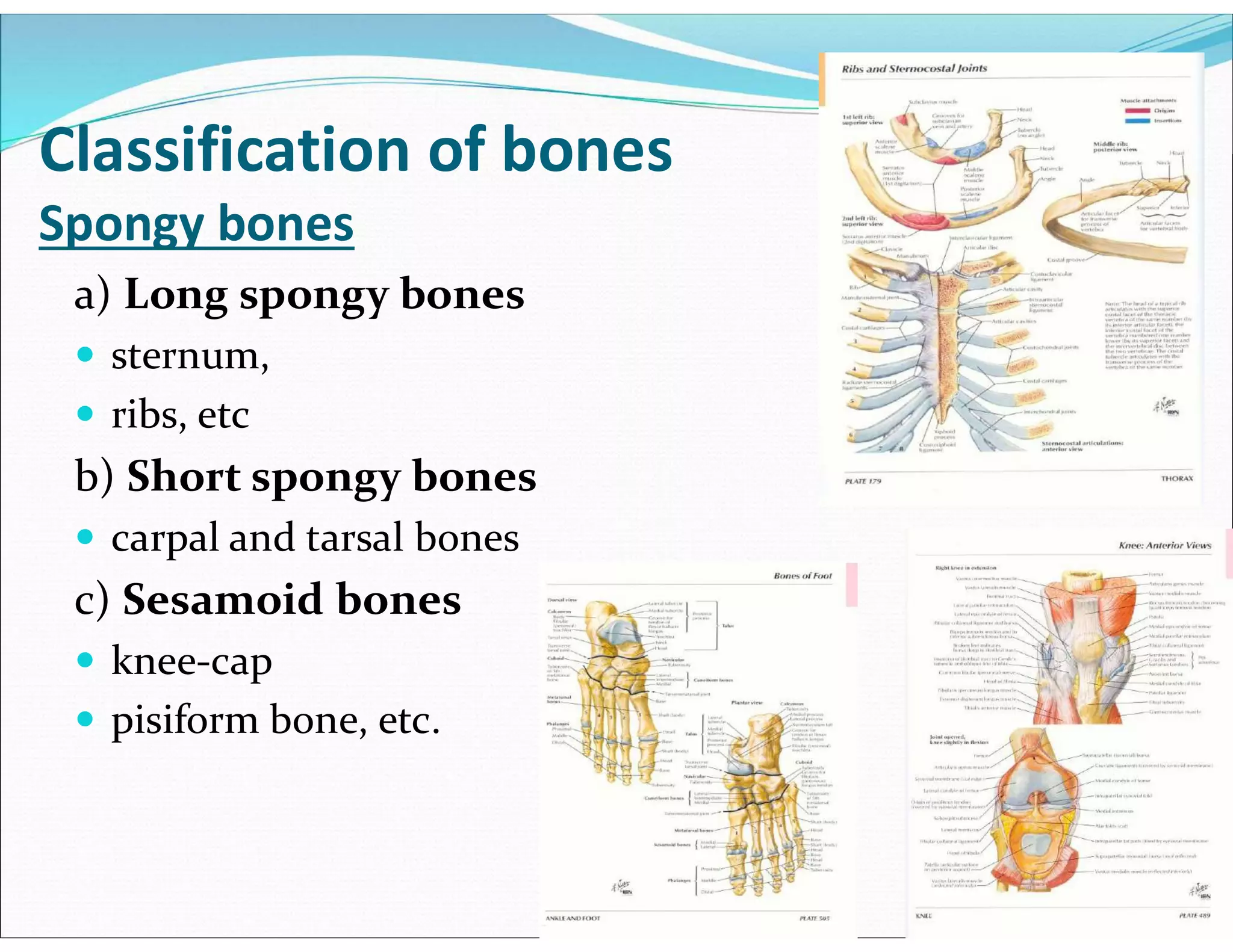
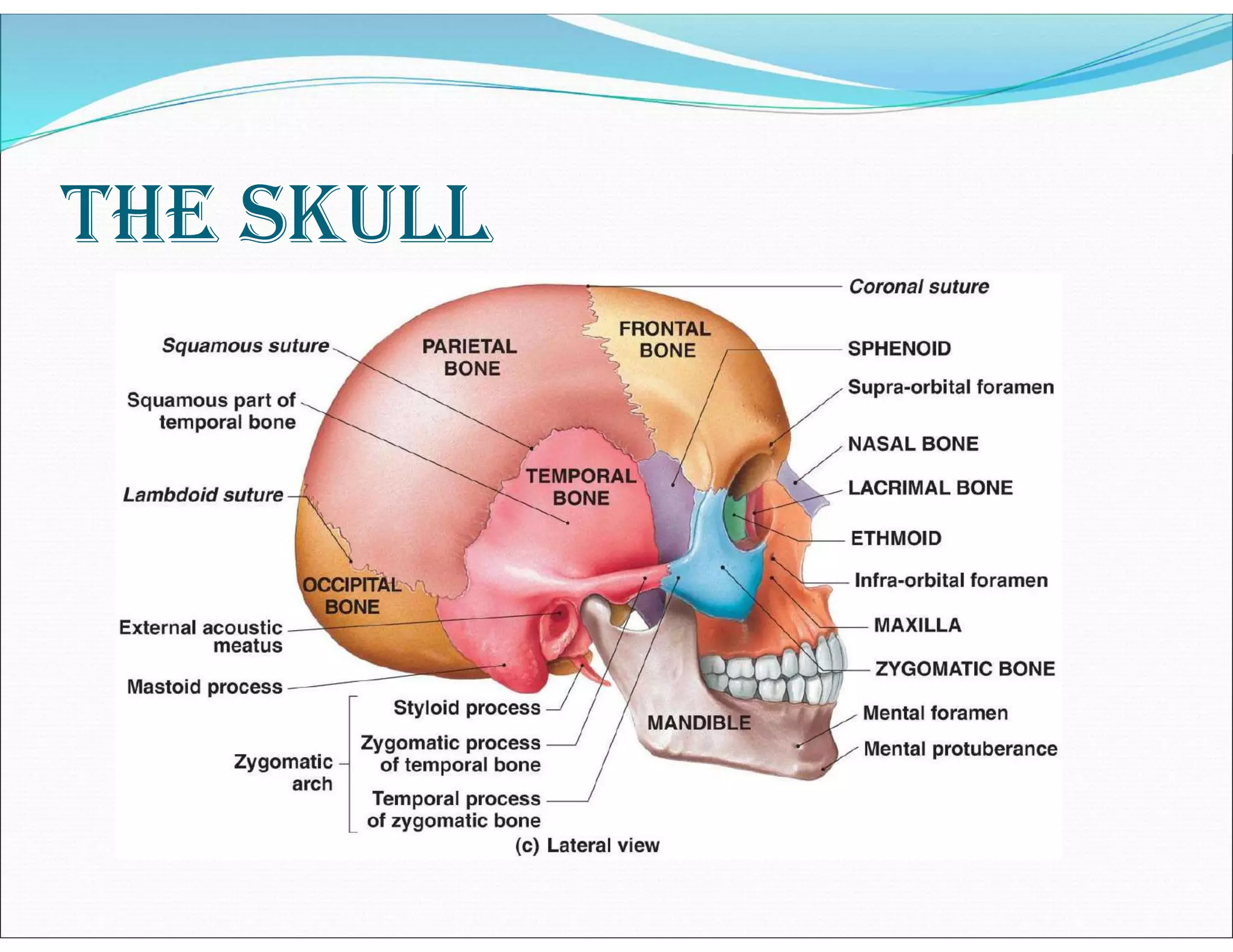
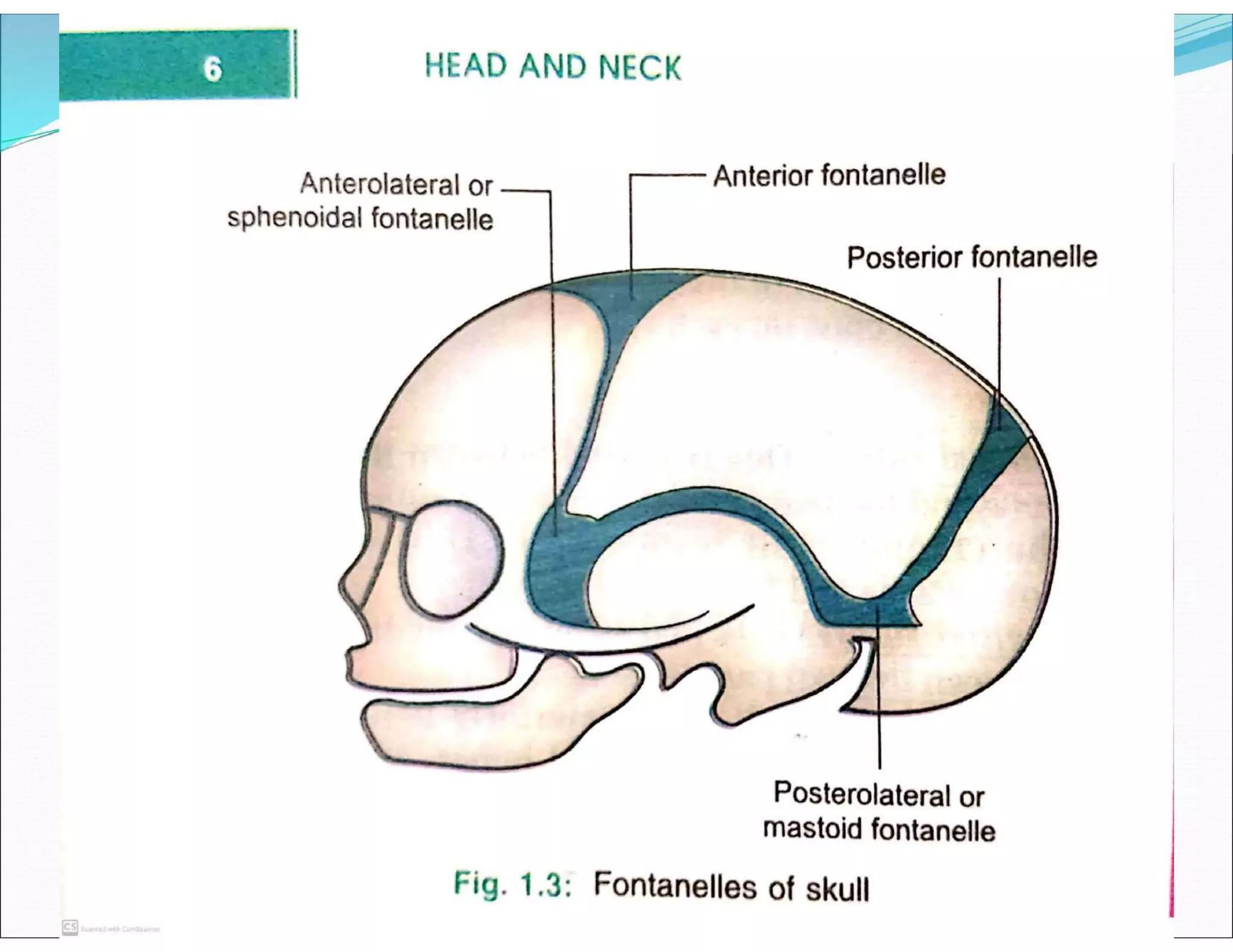
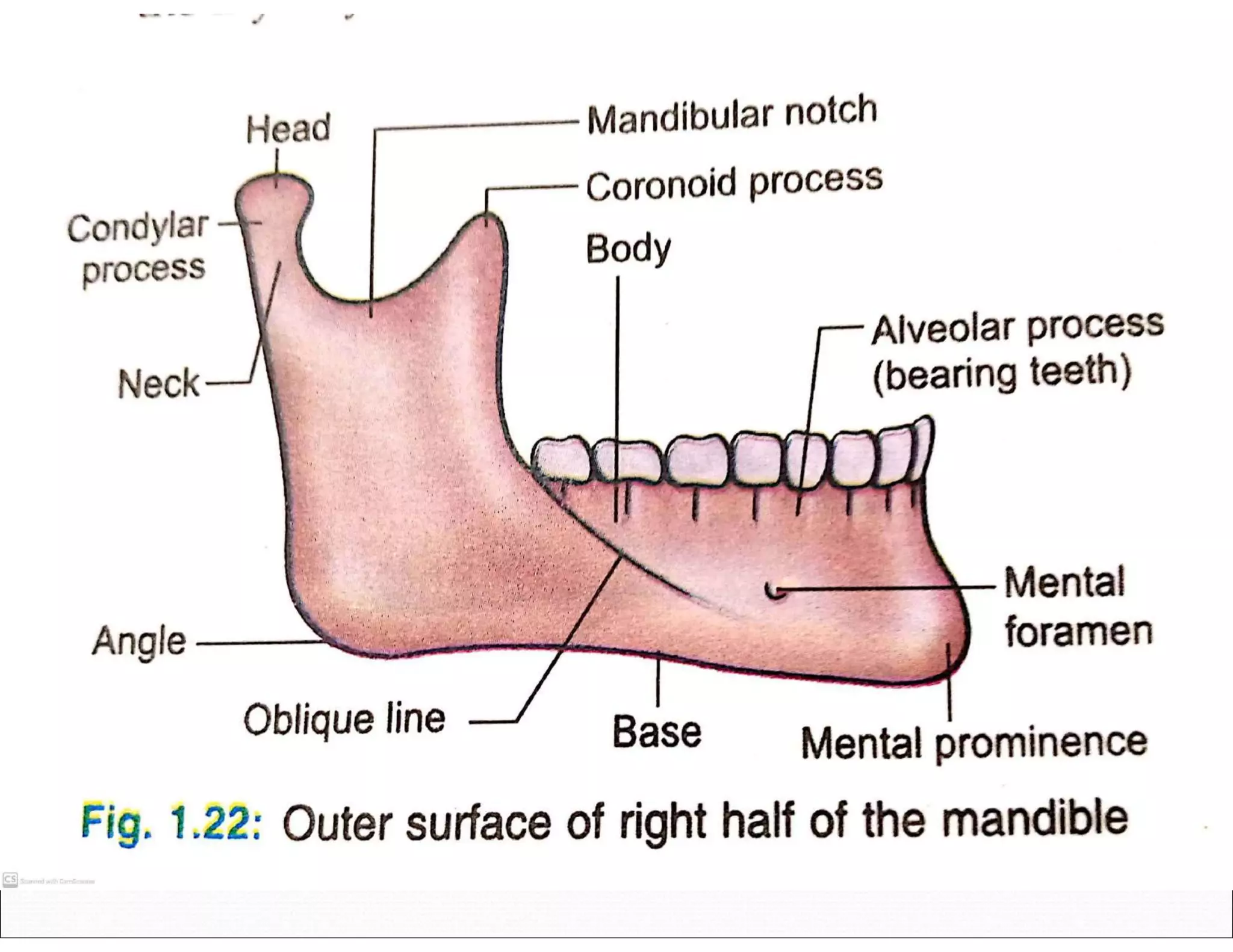
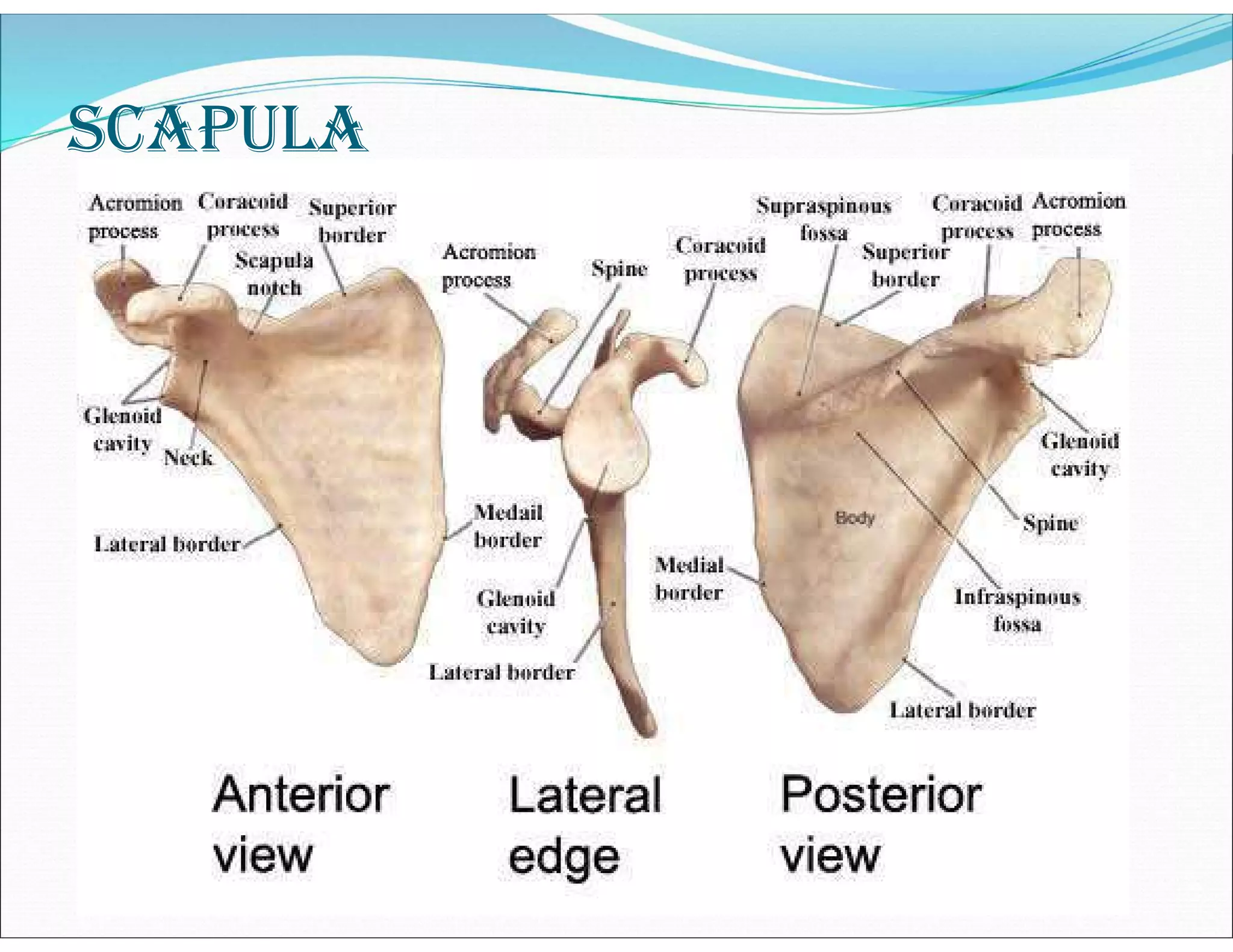
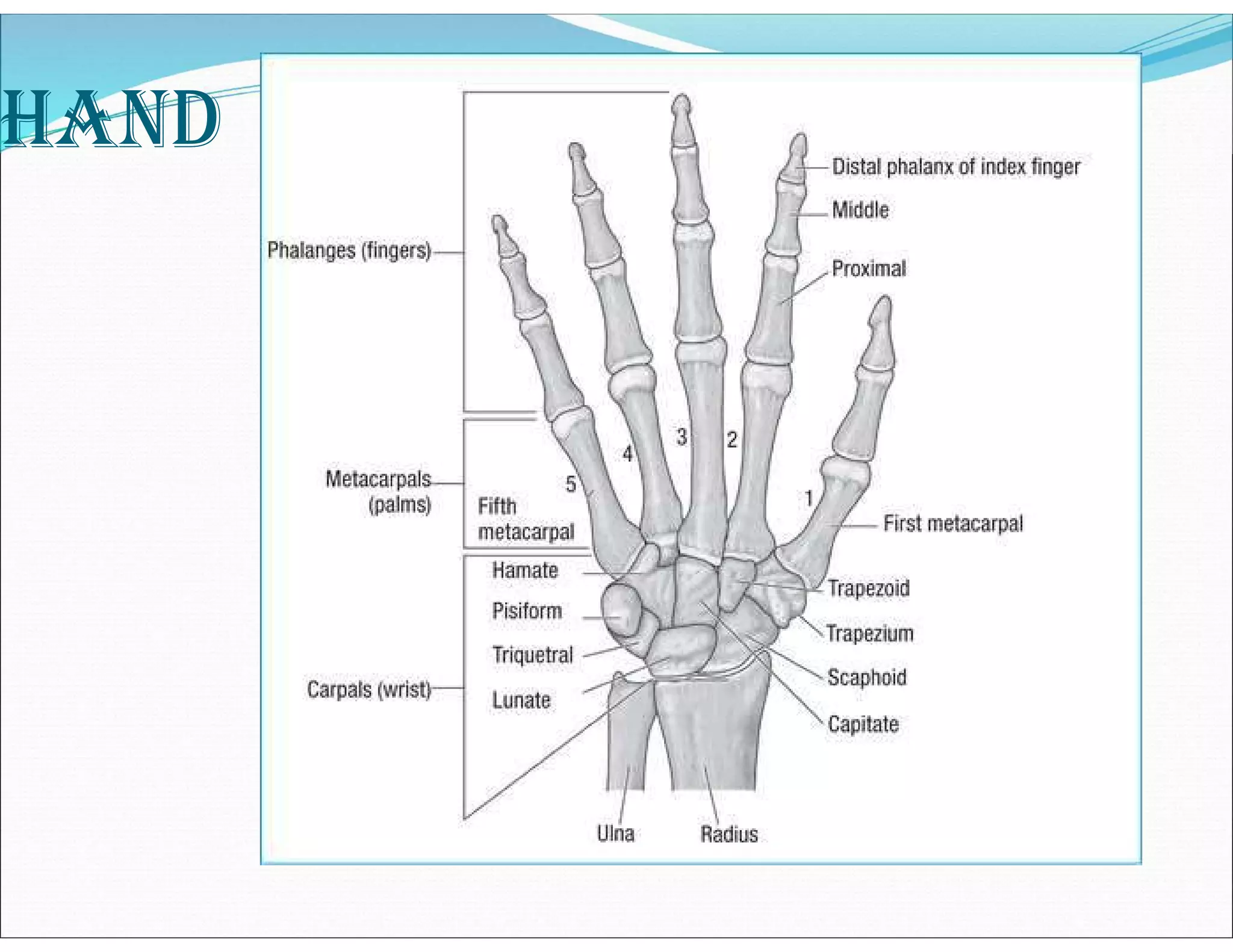
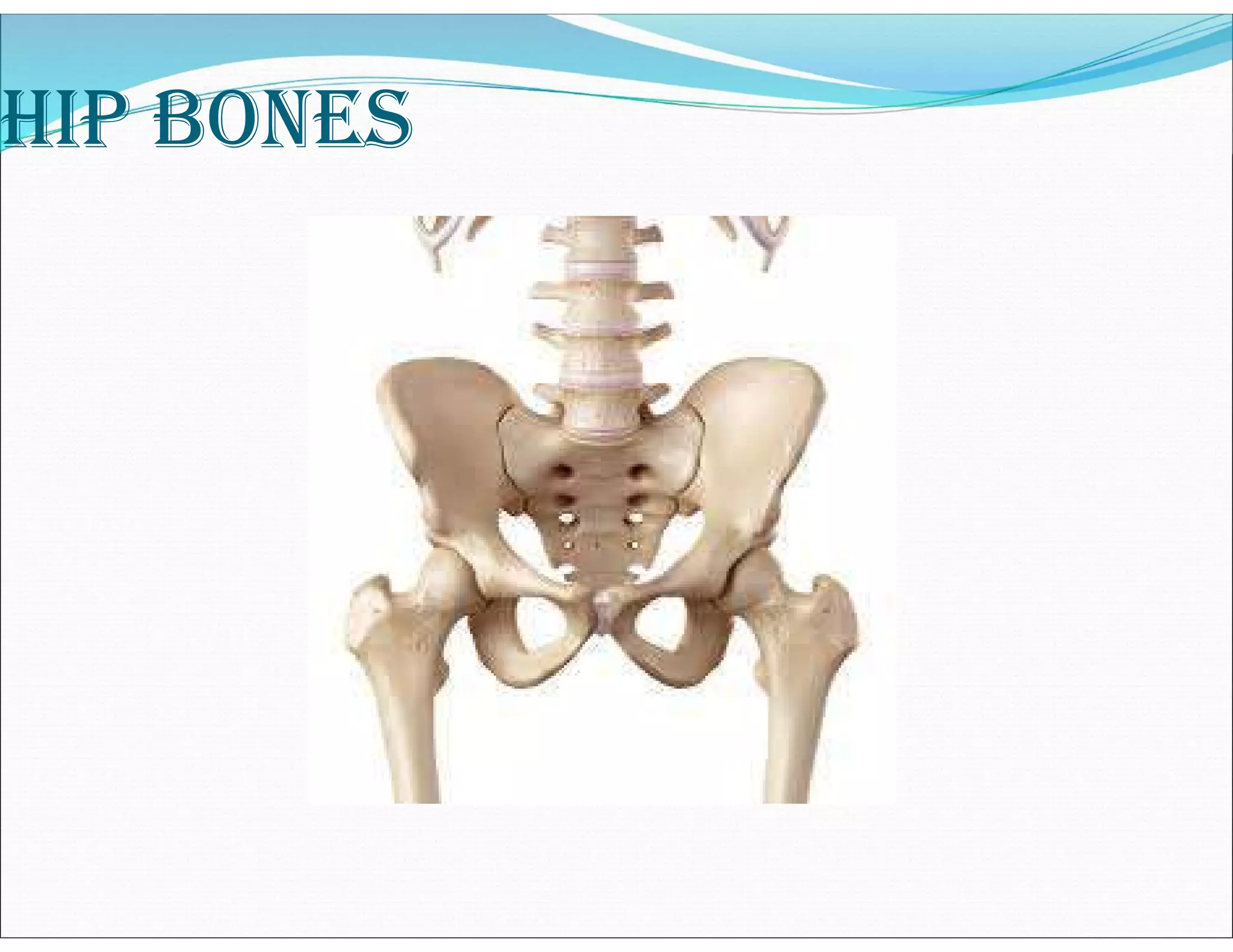
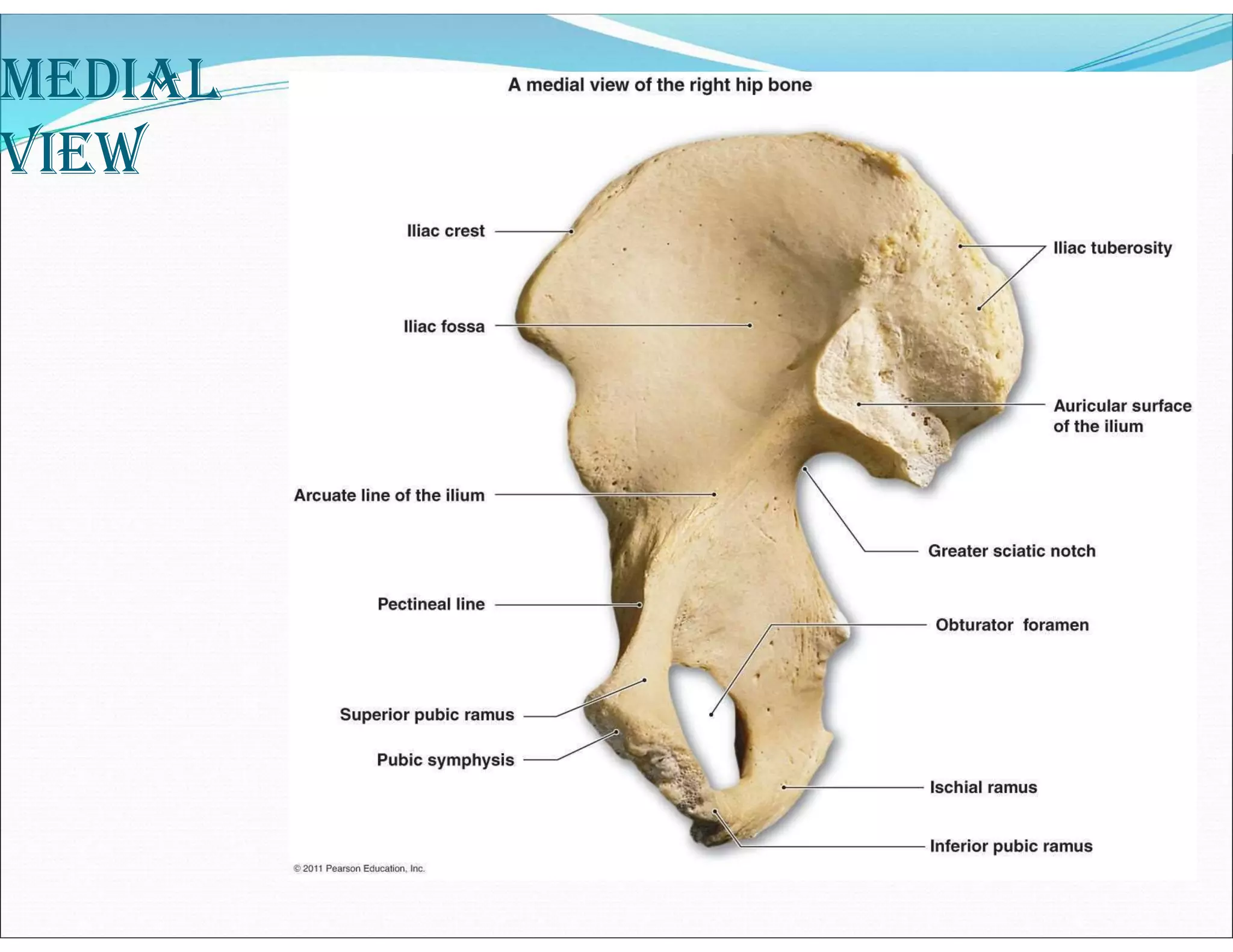
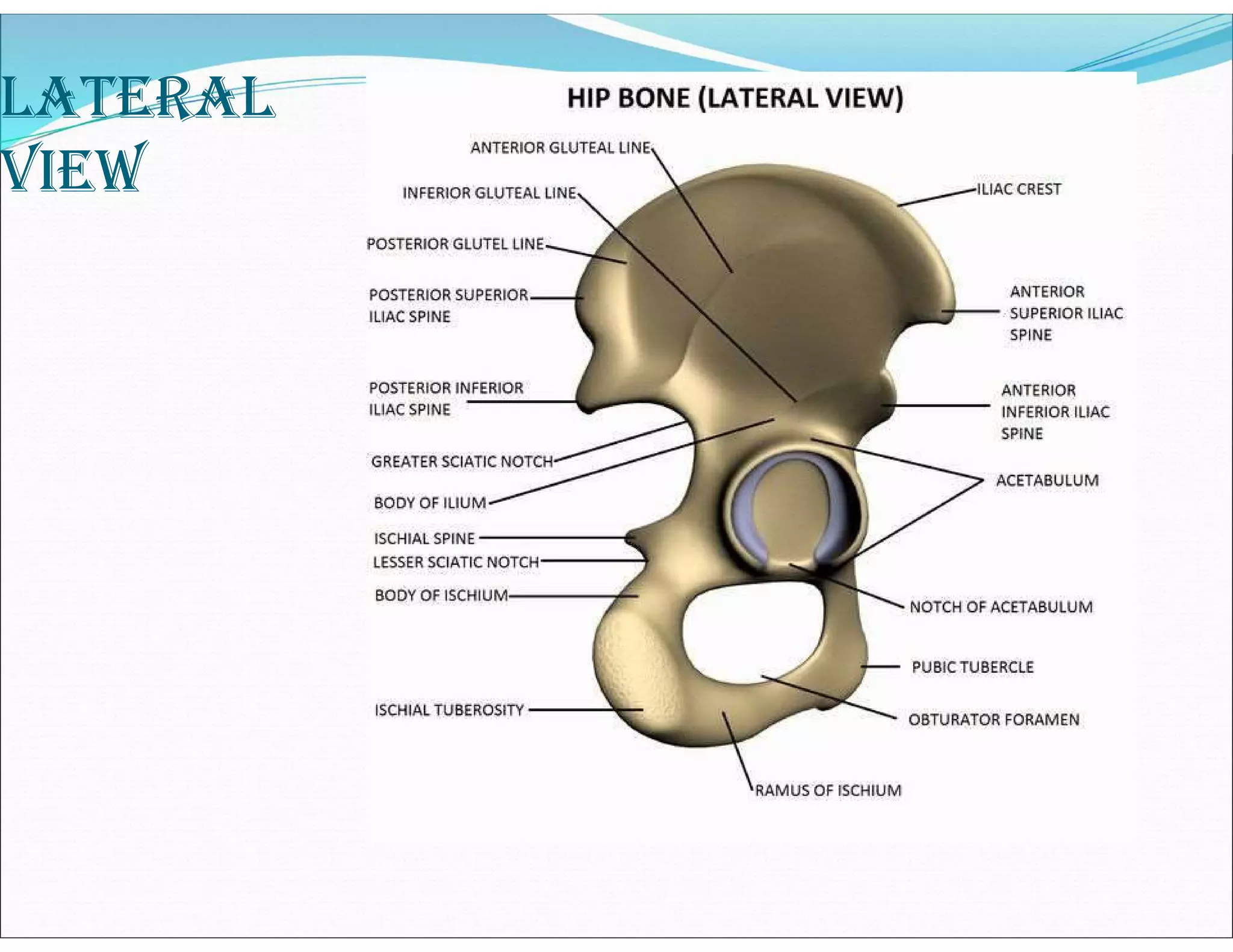
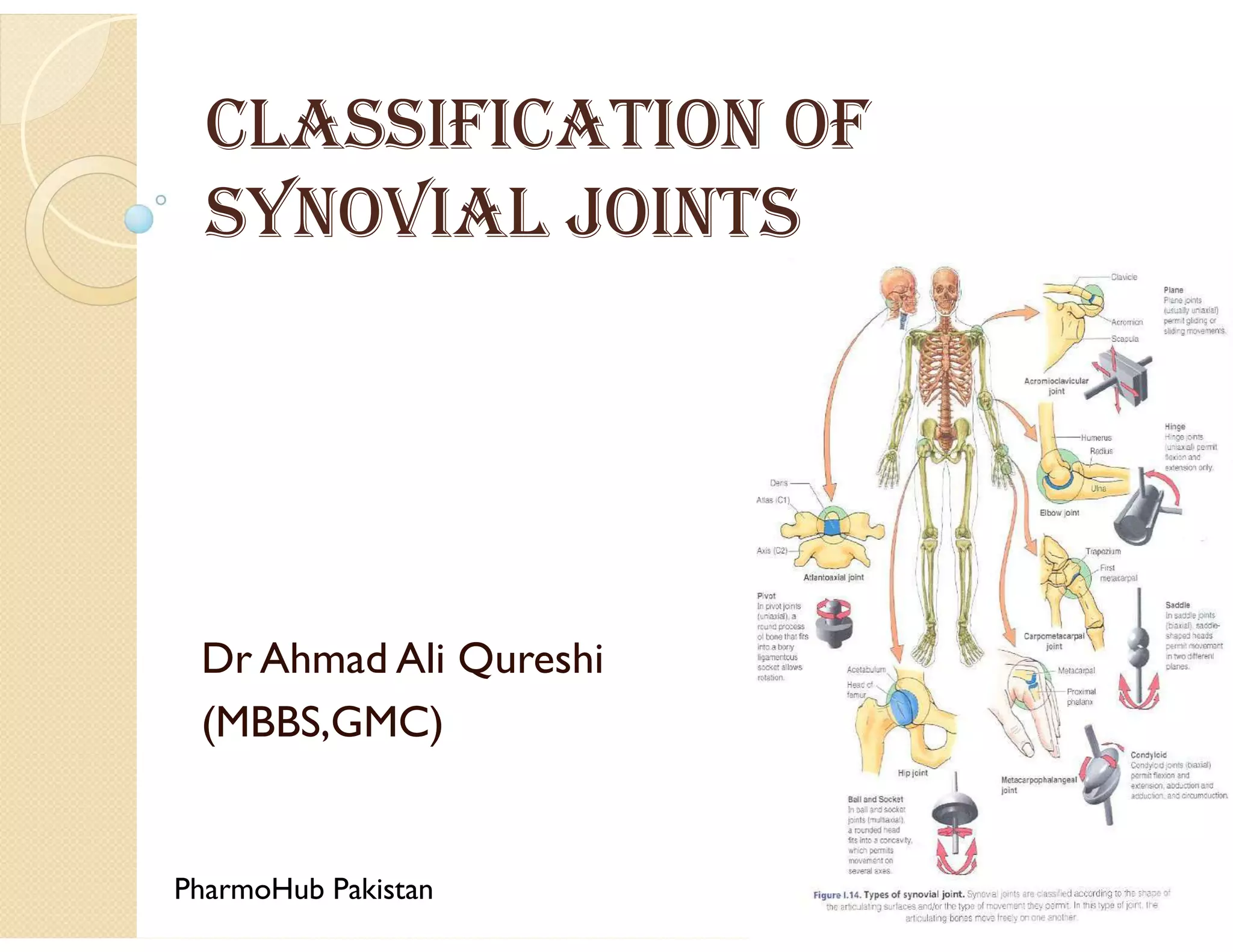
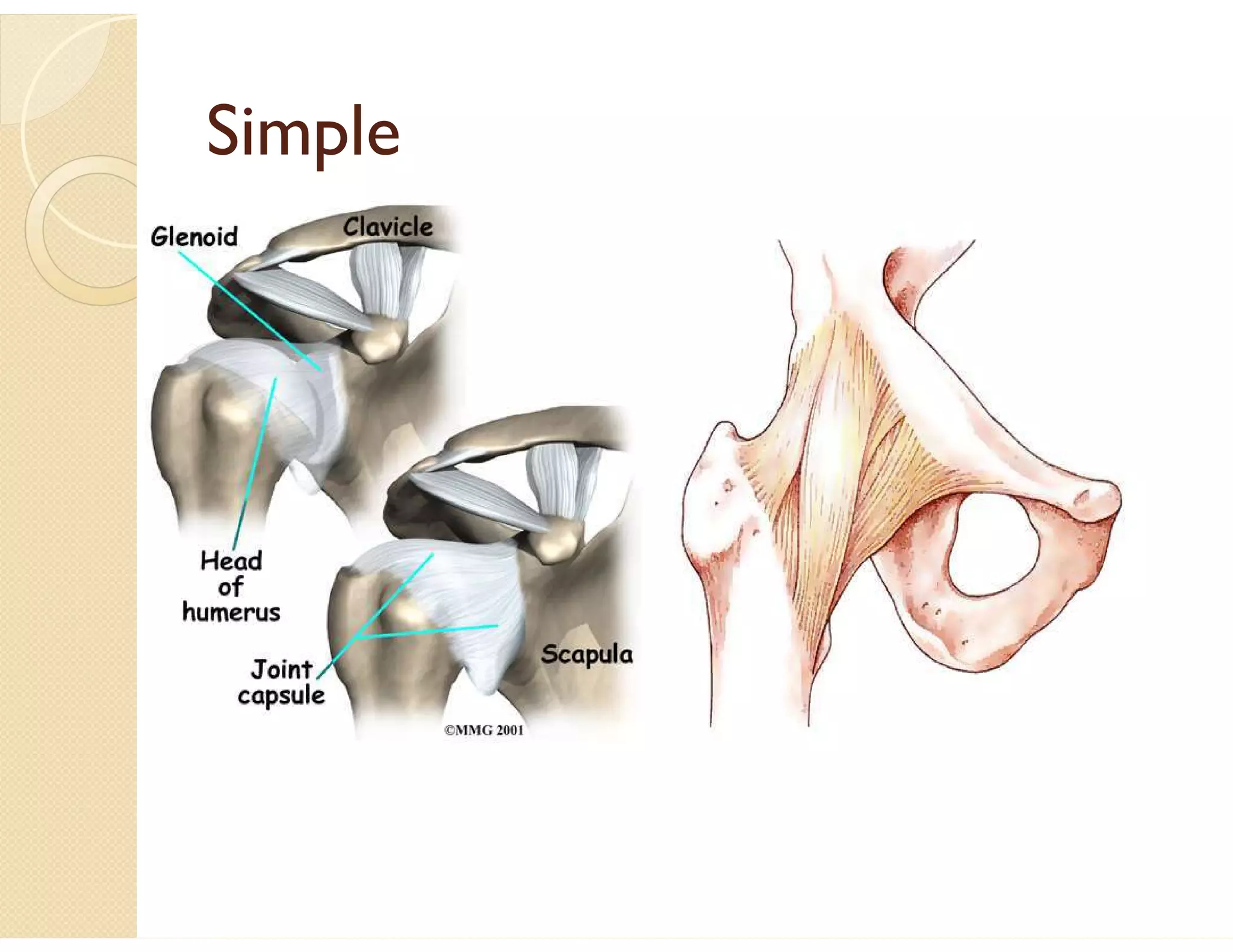
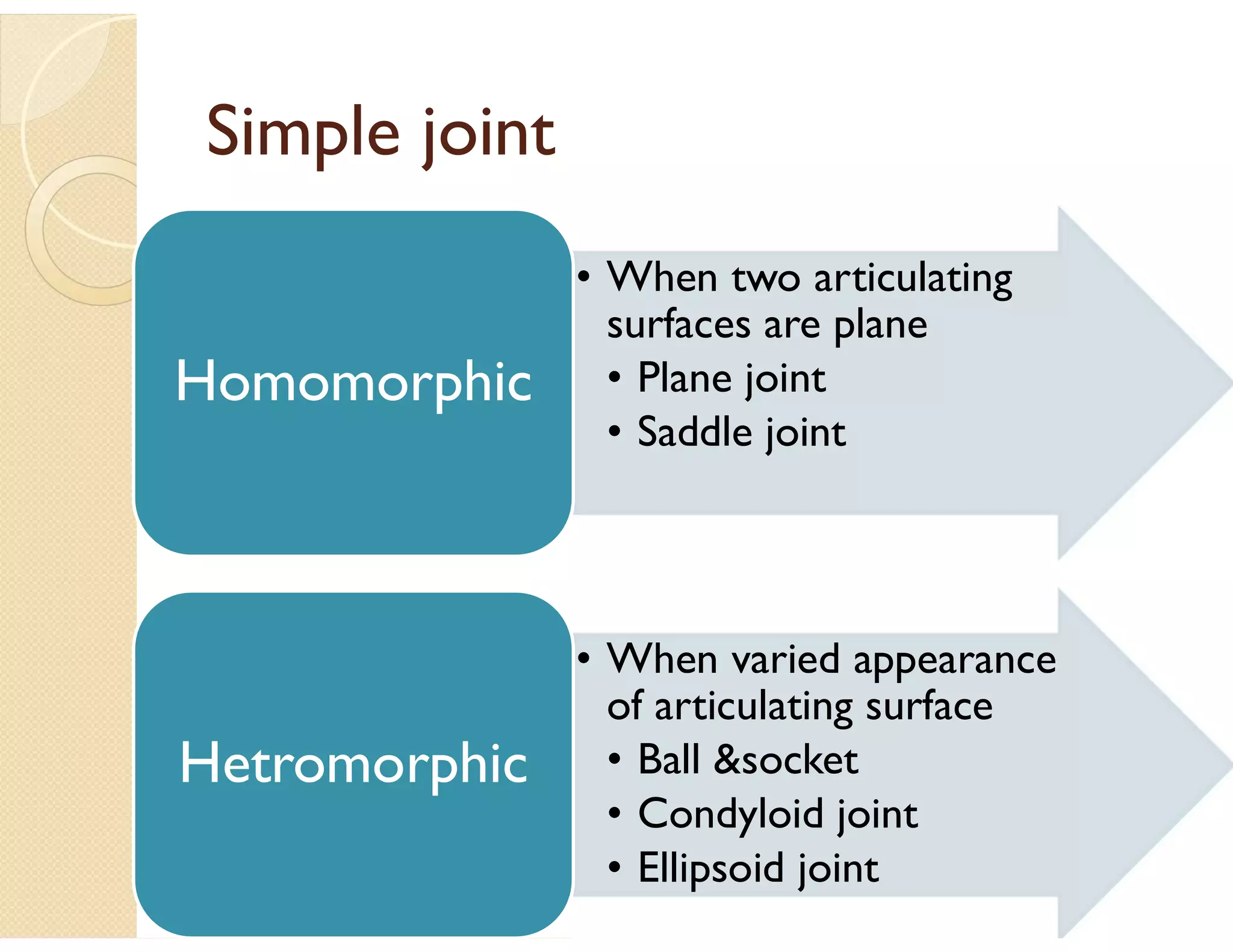
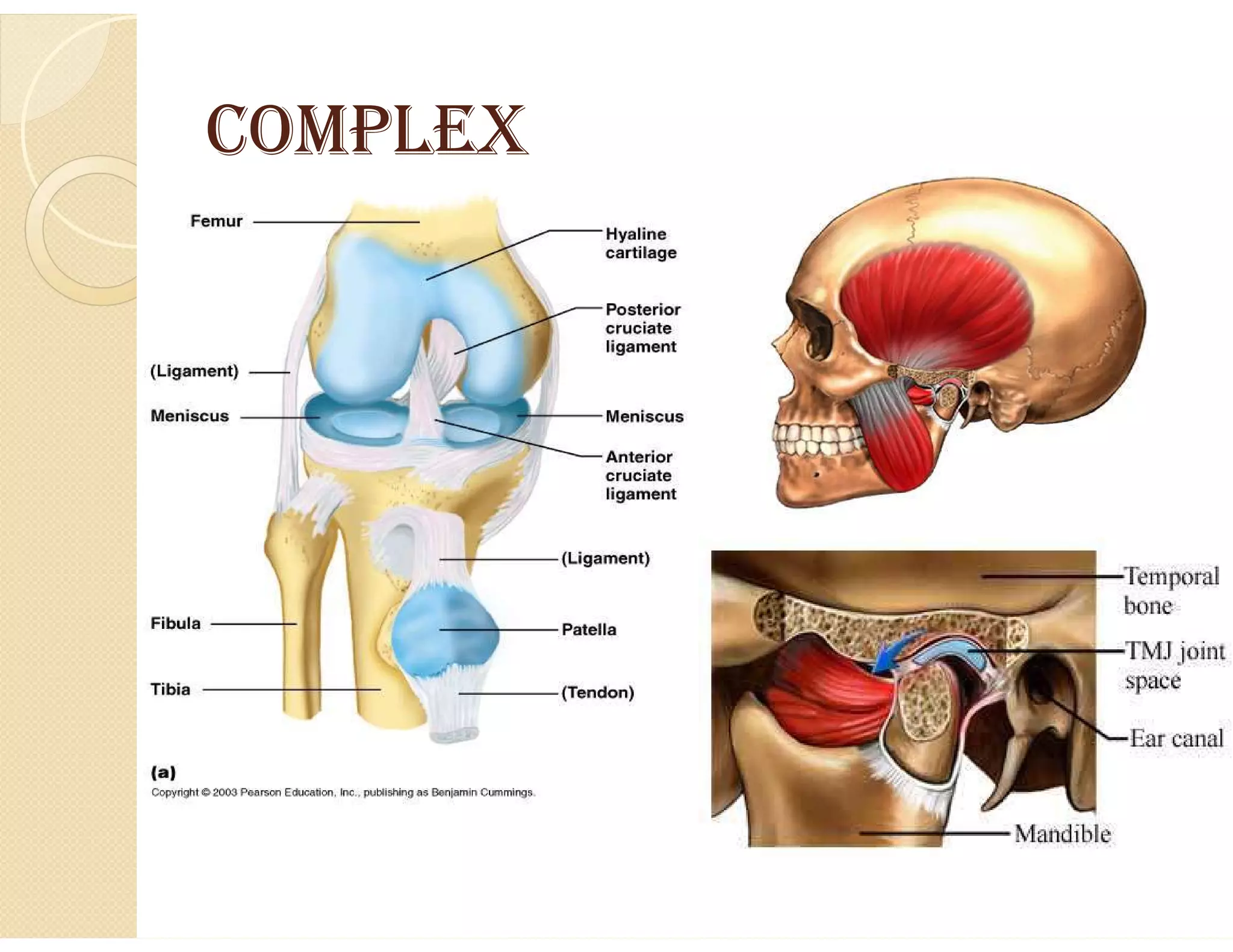
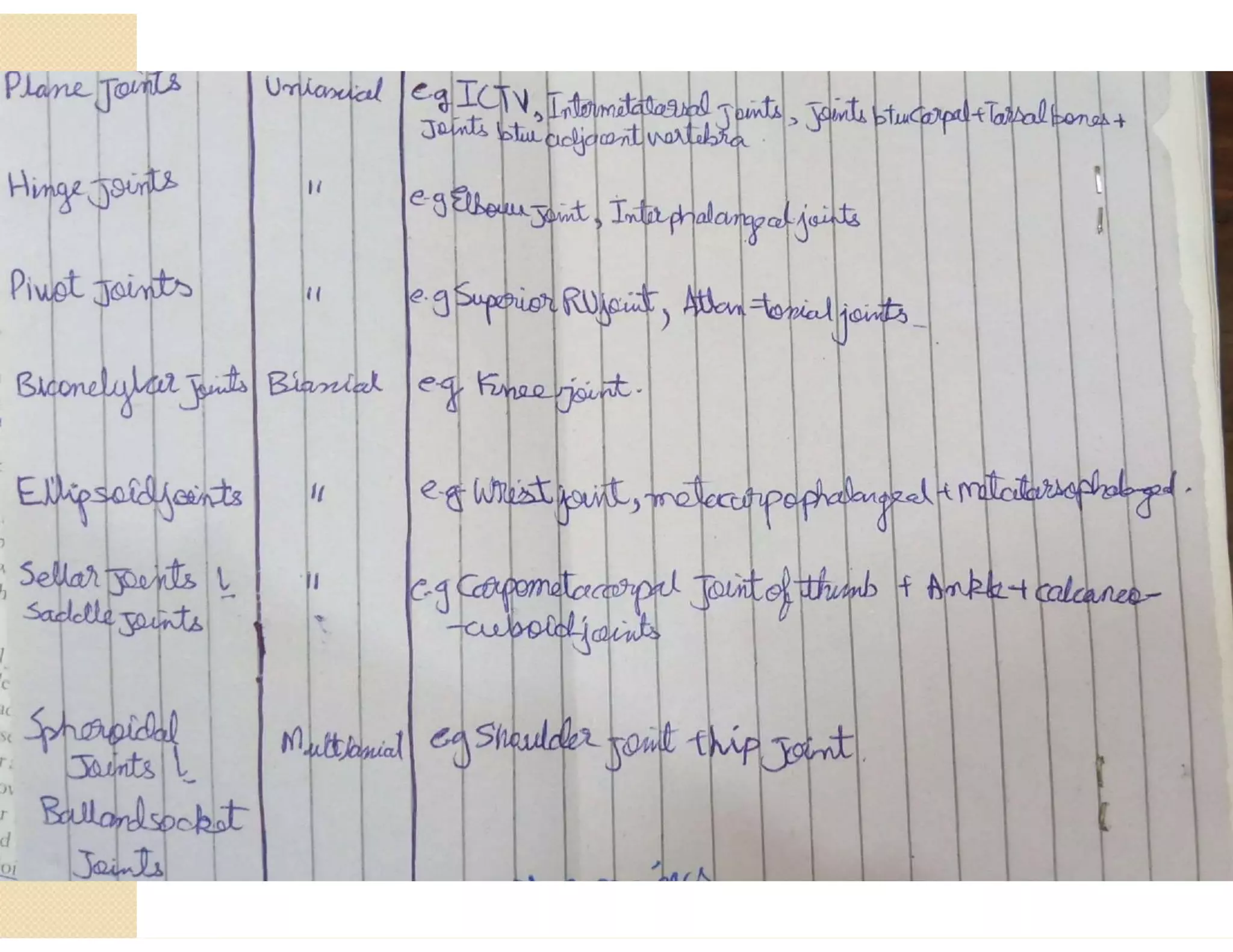
In-depth examination of the skeleton, its components, classifications, and functions in human anatomy.
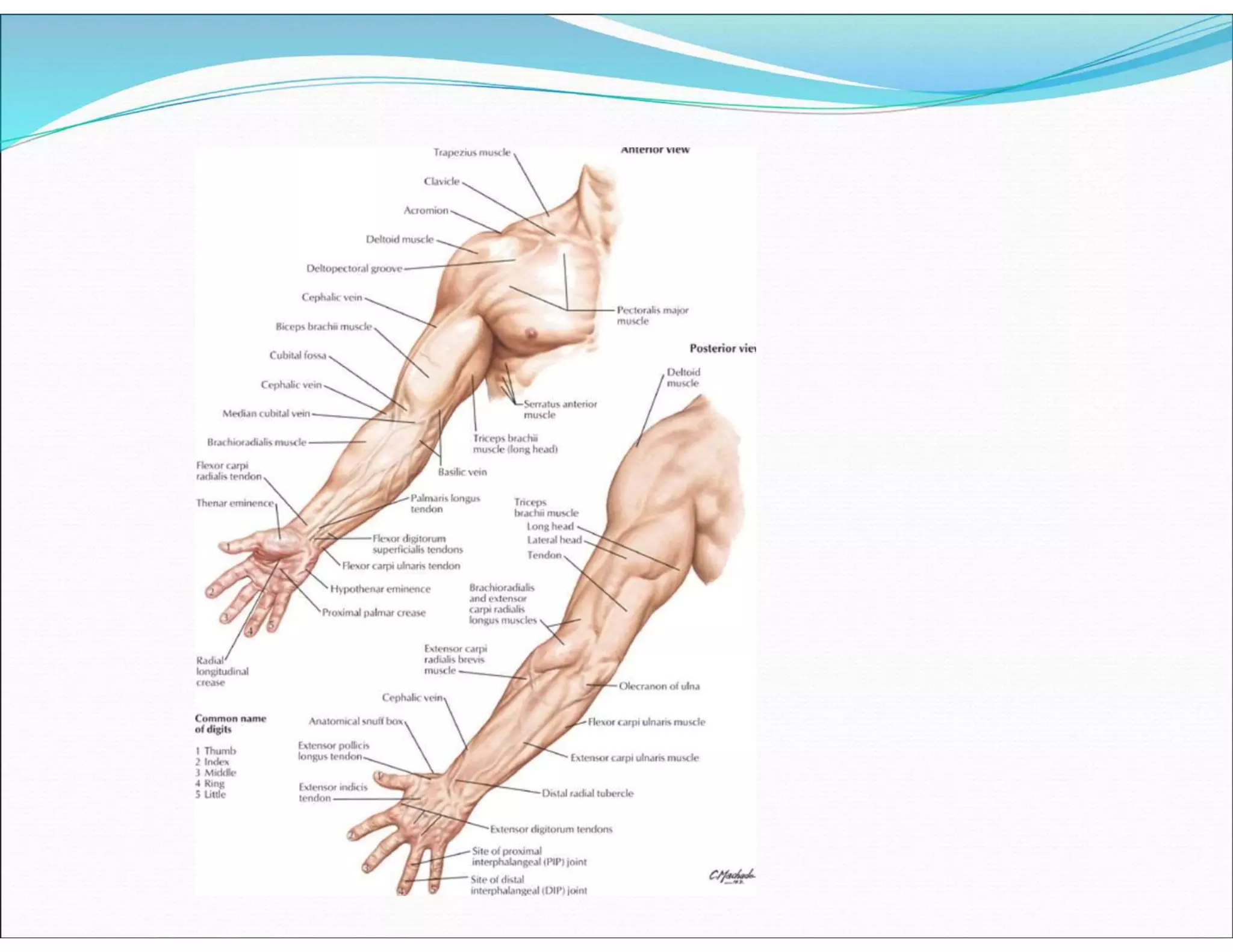
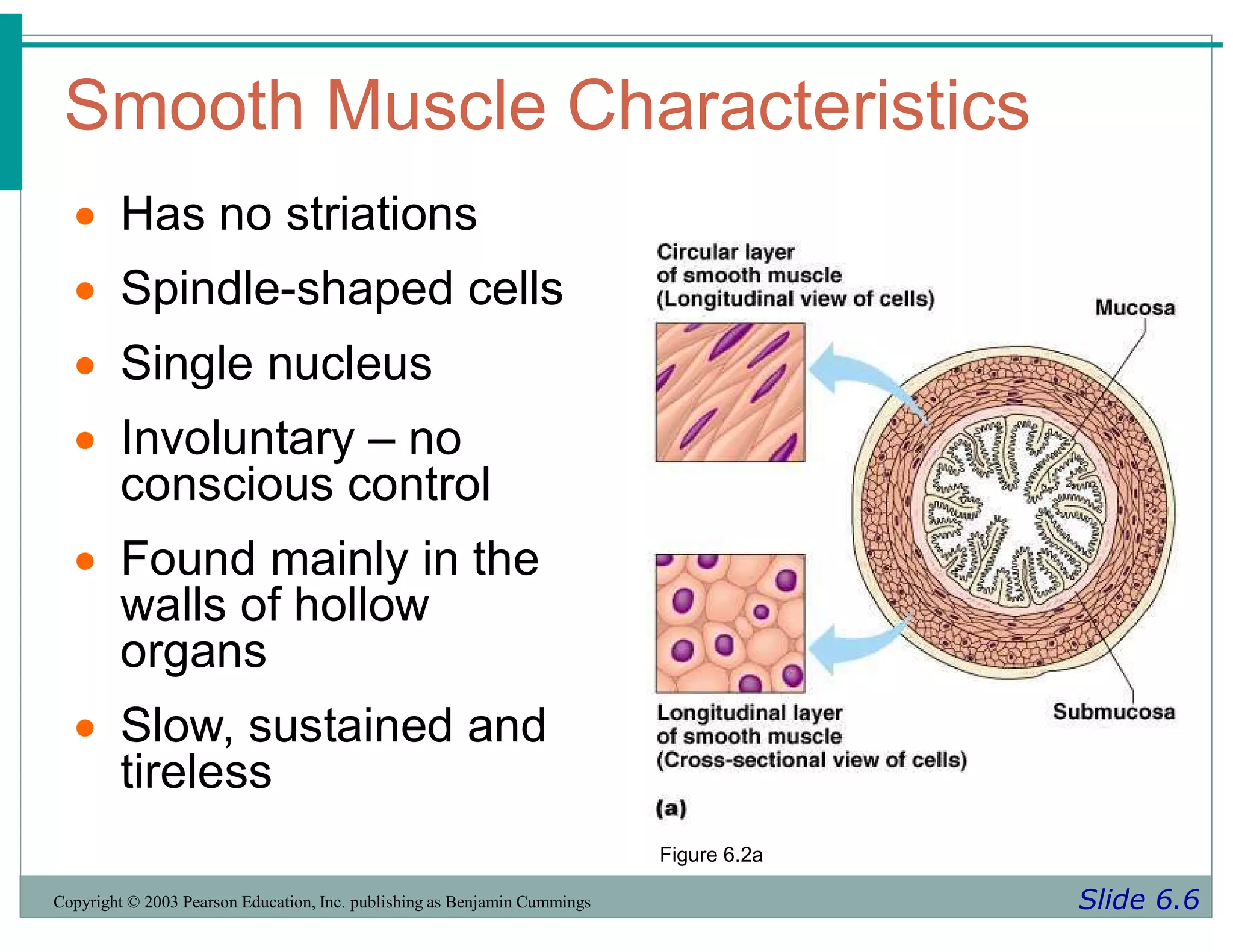
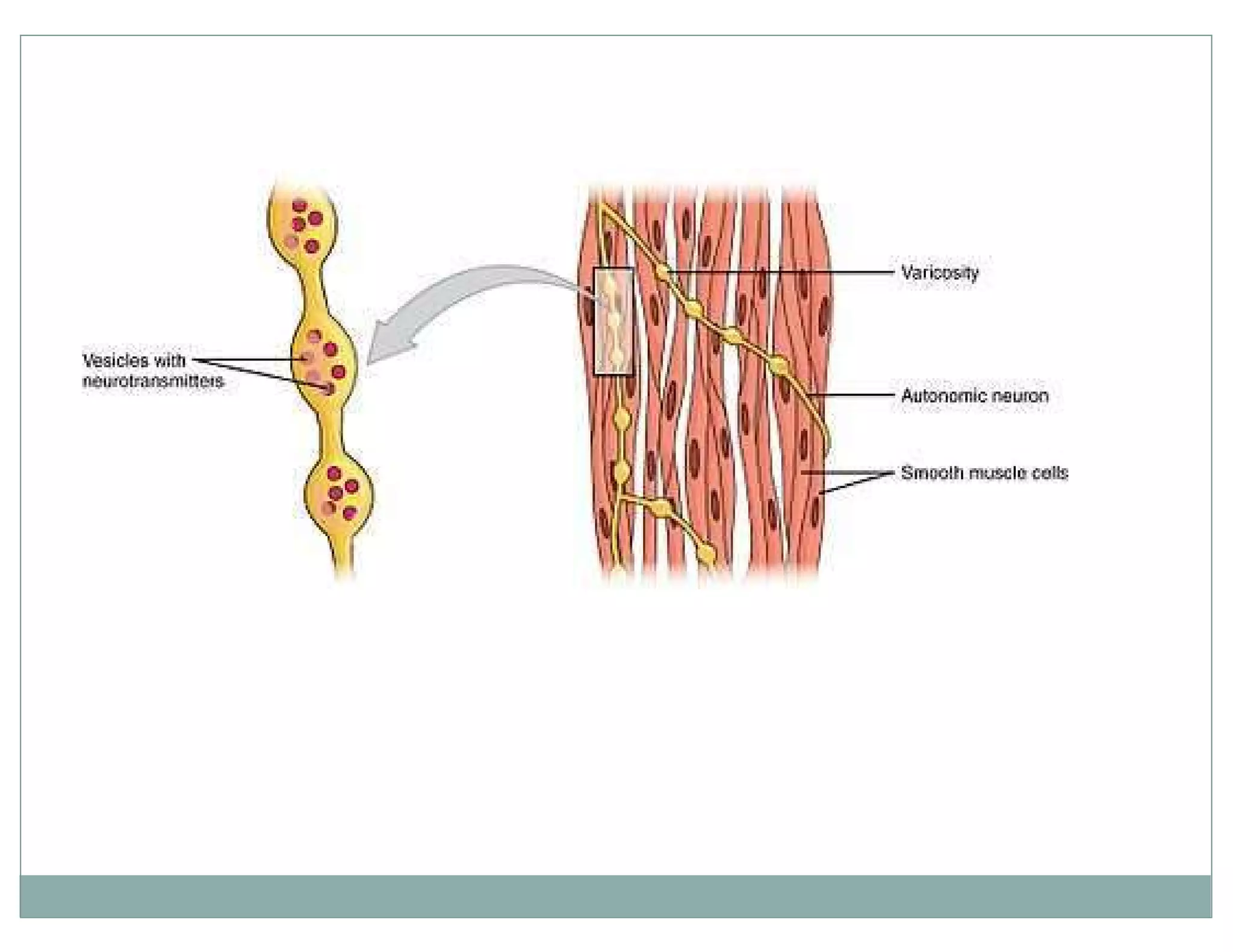
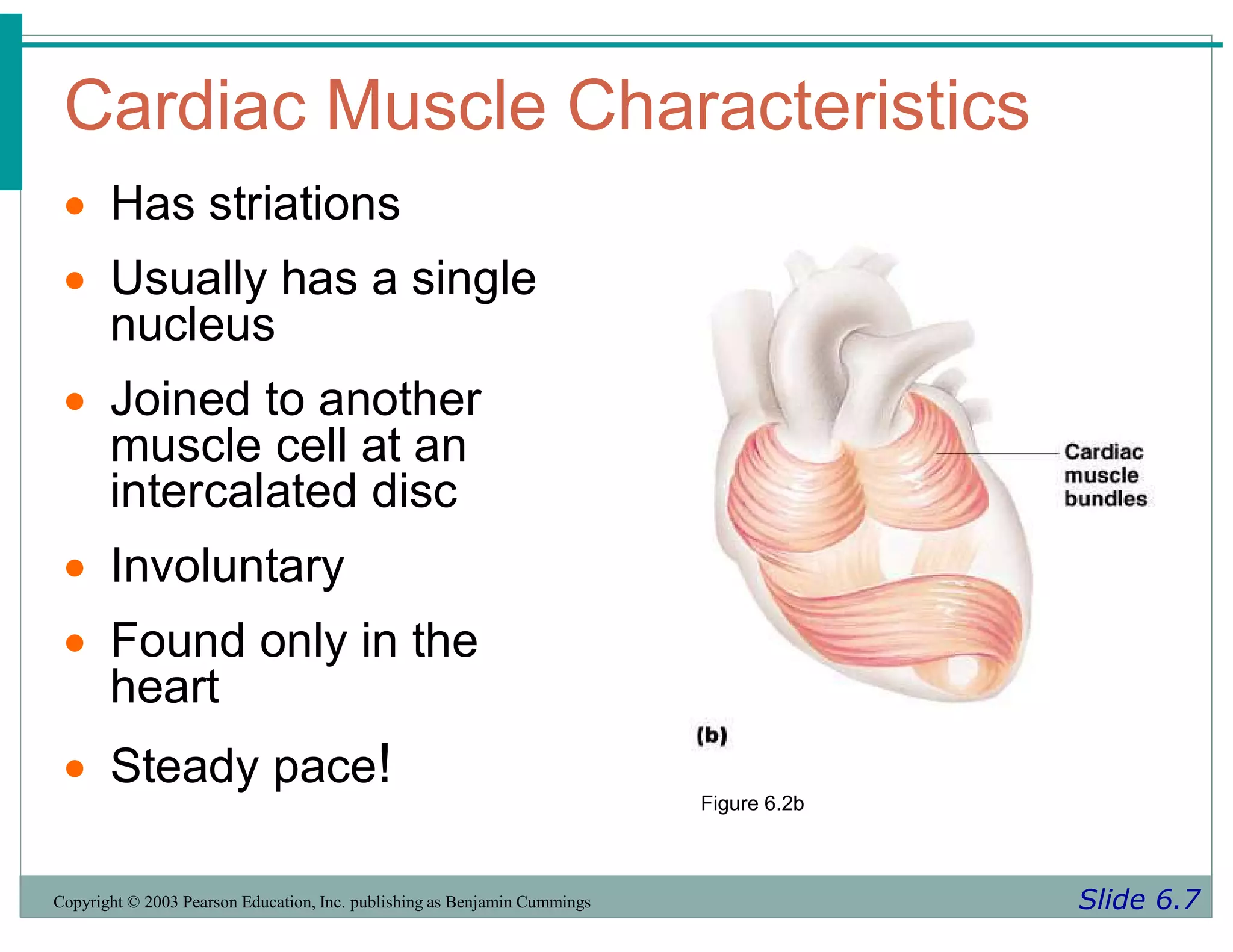
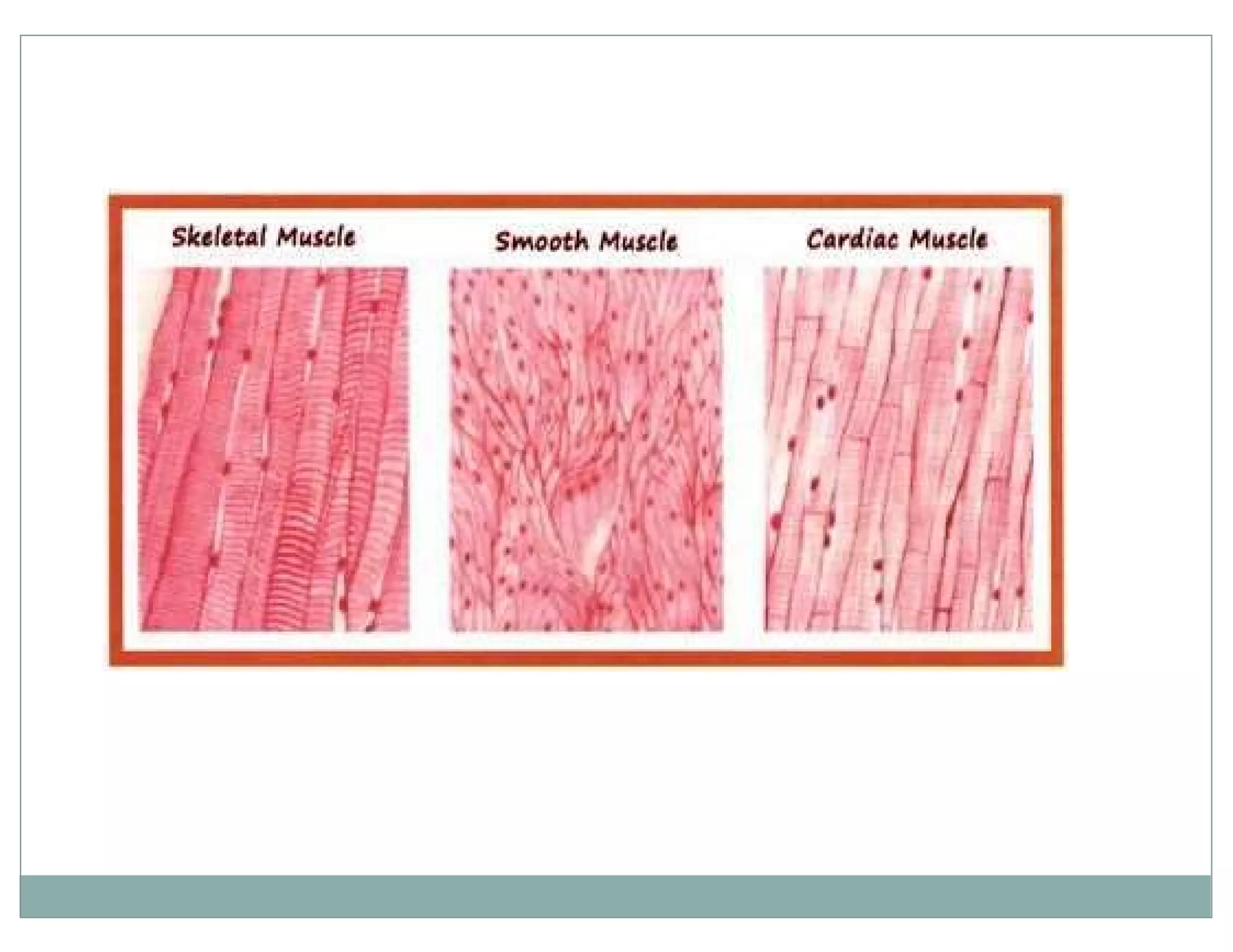
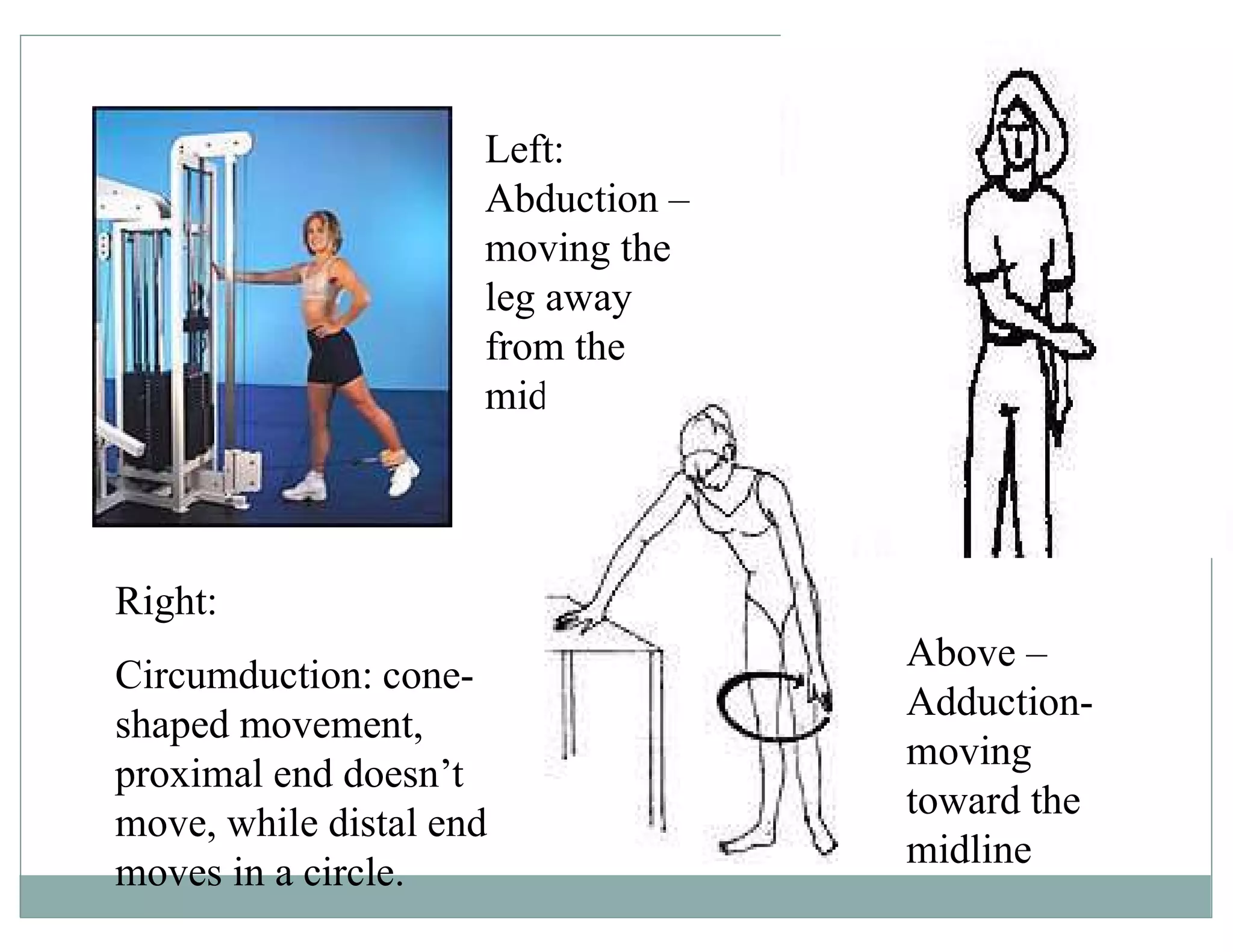
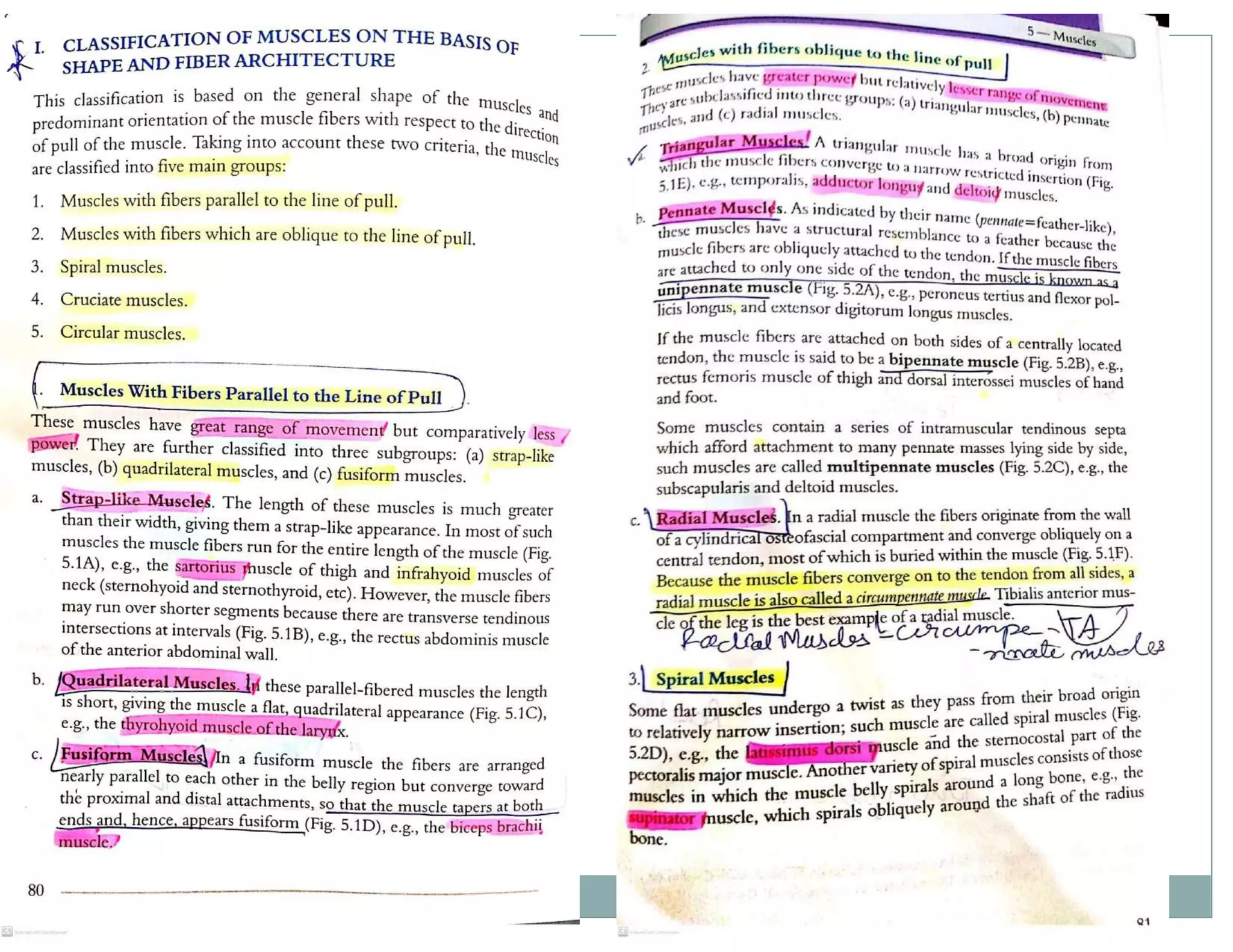
Overview of muscular anatomy, types of muscles, and their functions related to movement and posture.
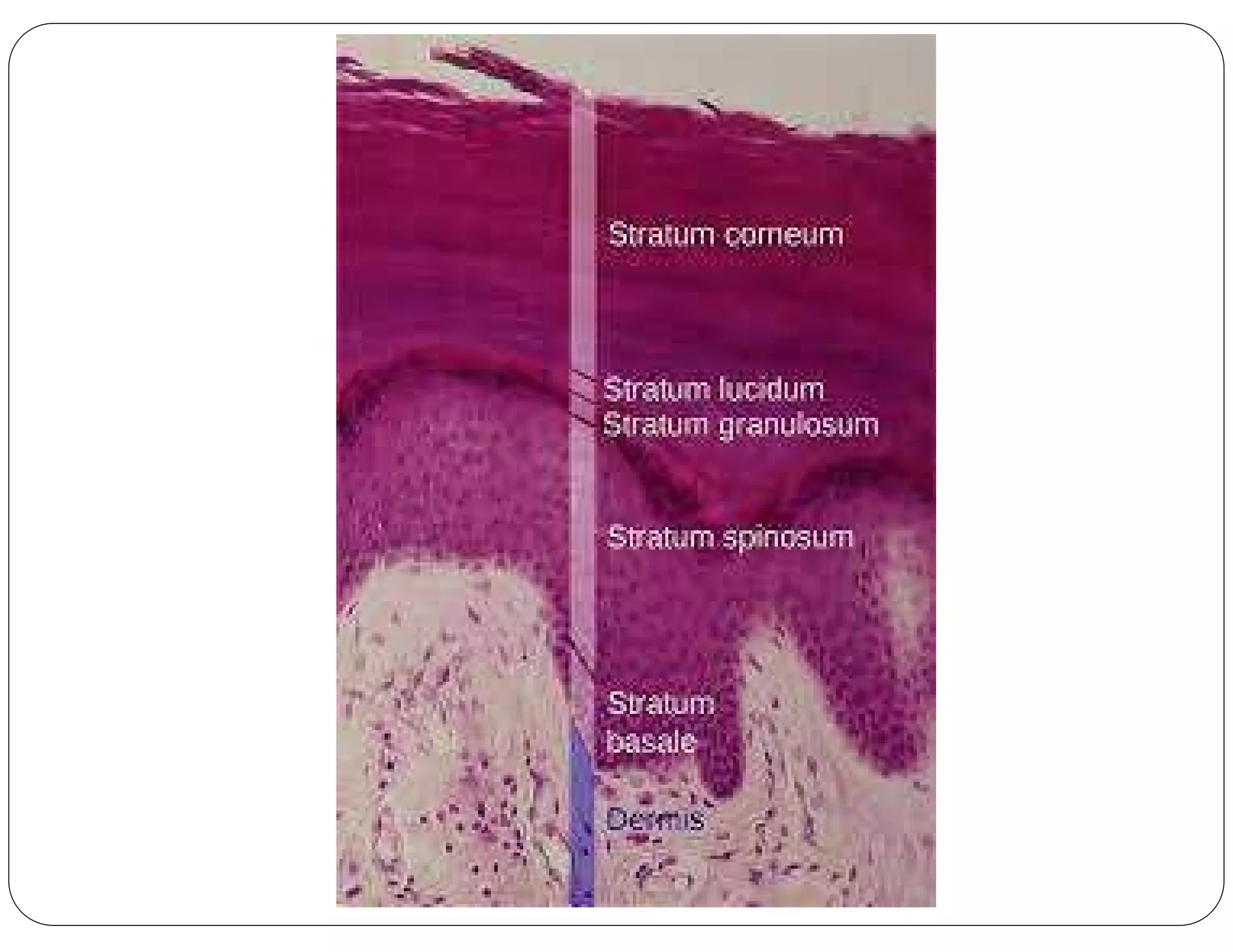
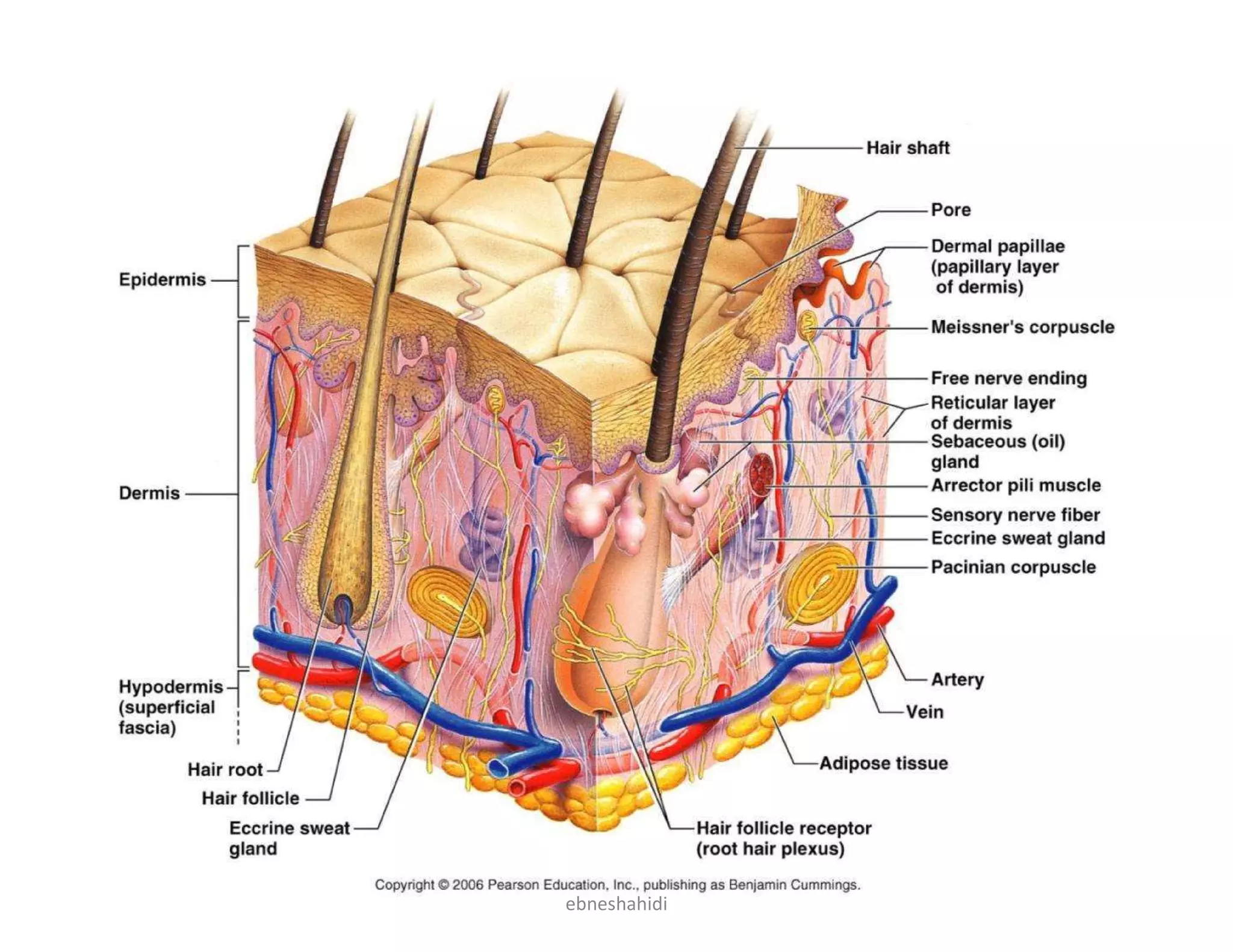
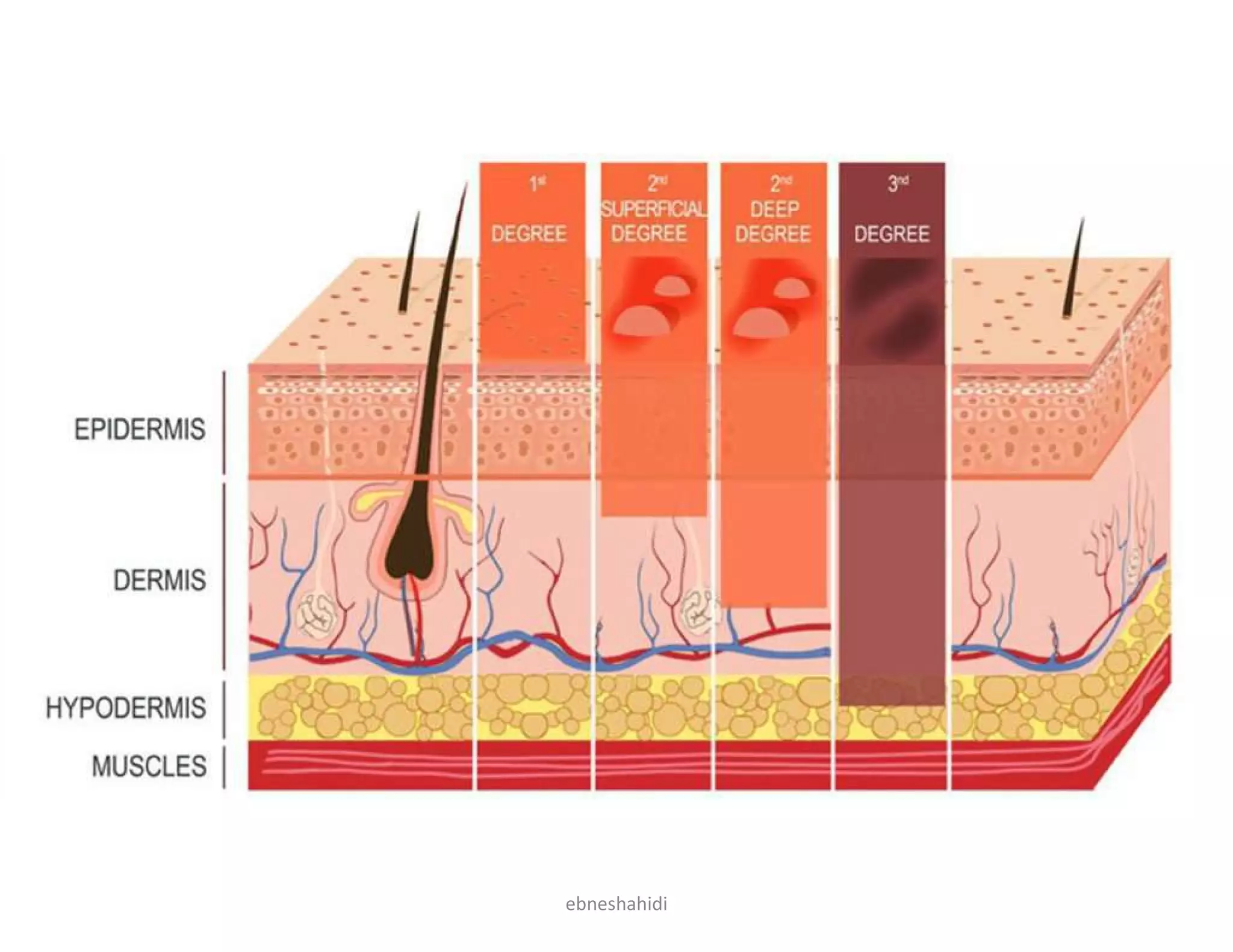
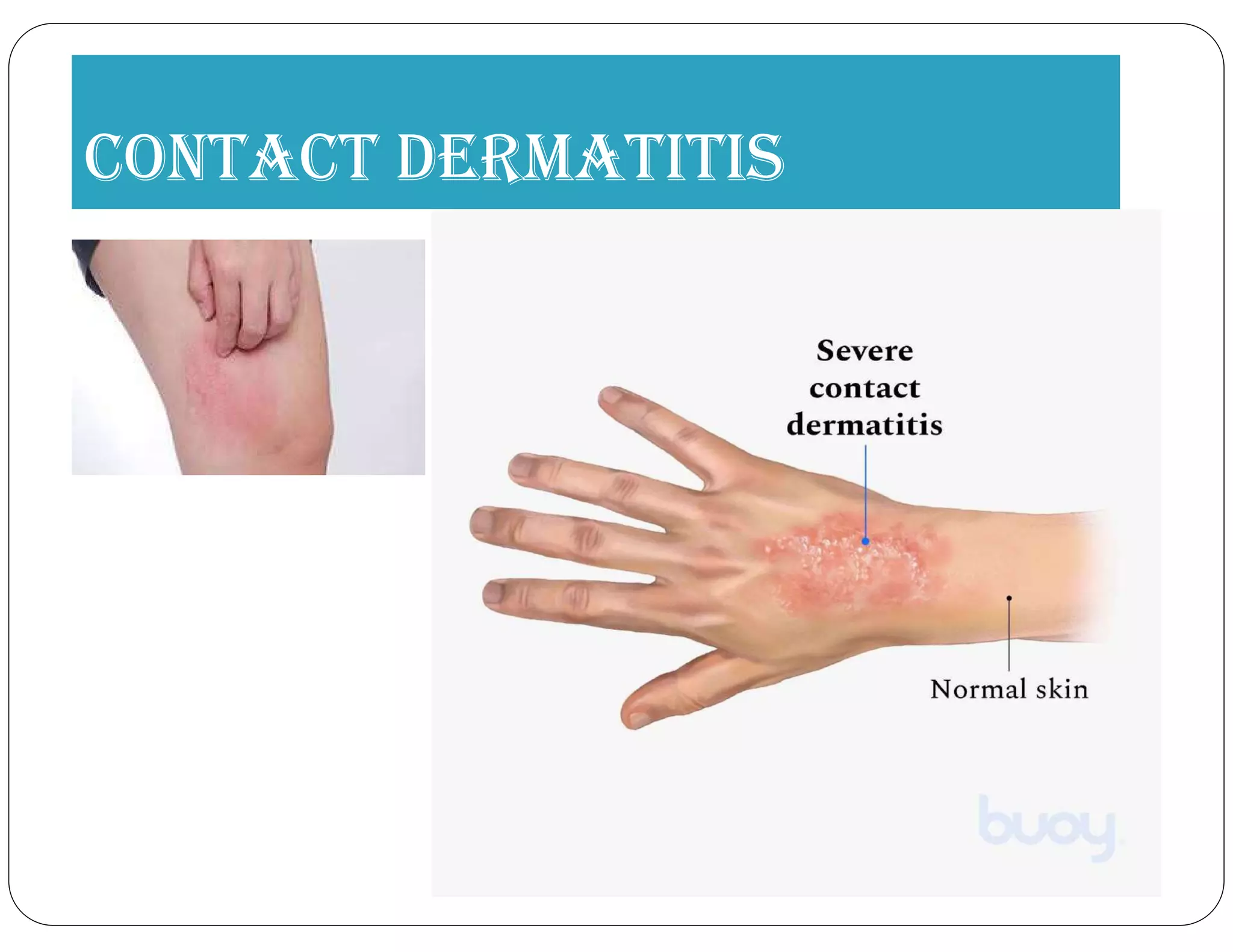
Details on skin anatomy, functions, and accessory structures.
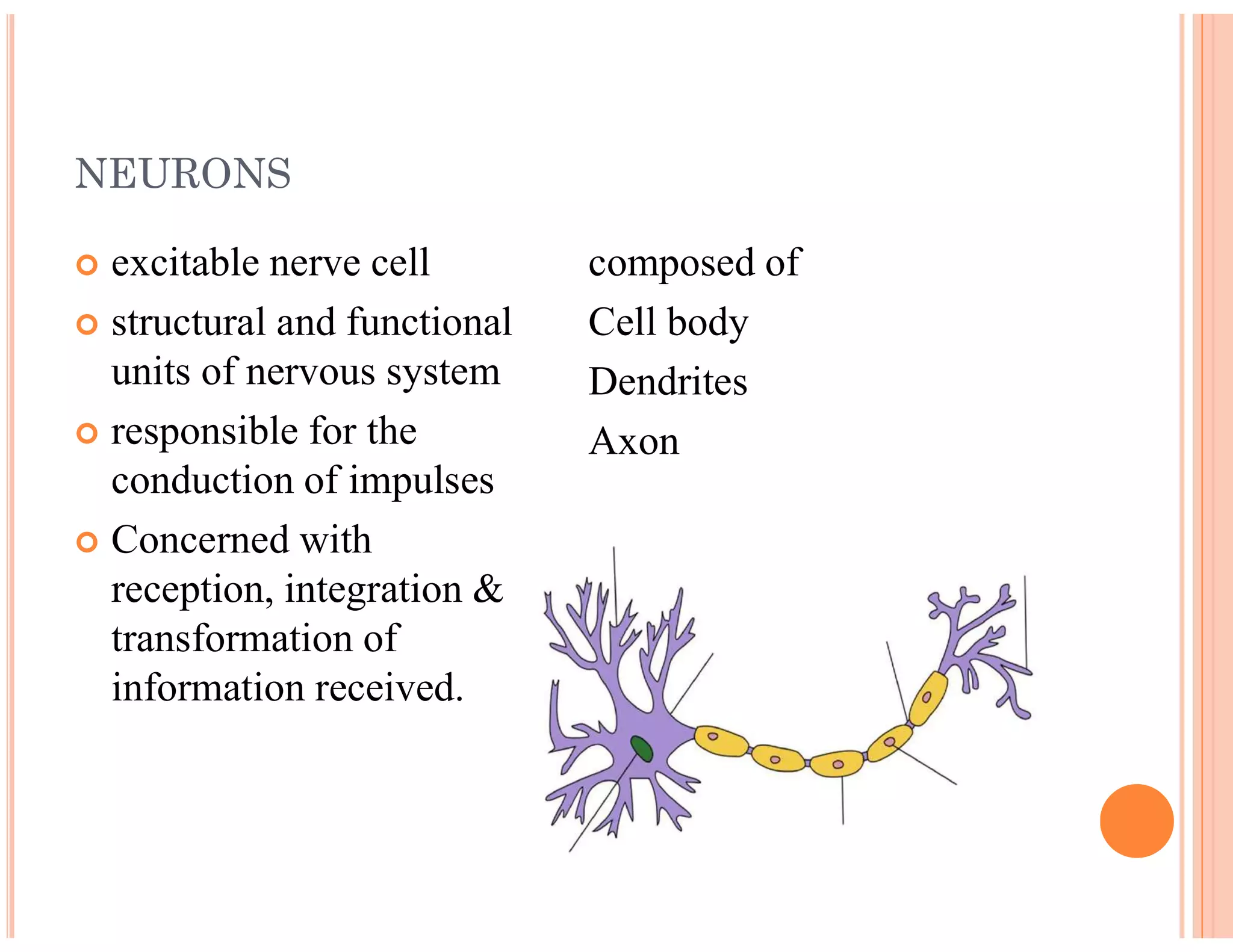
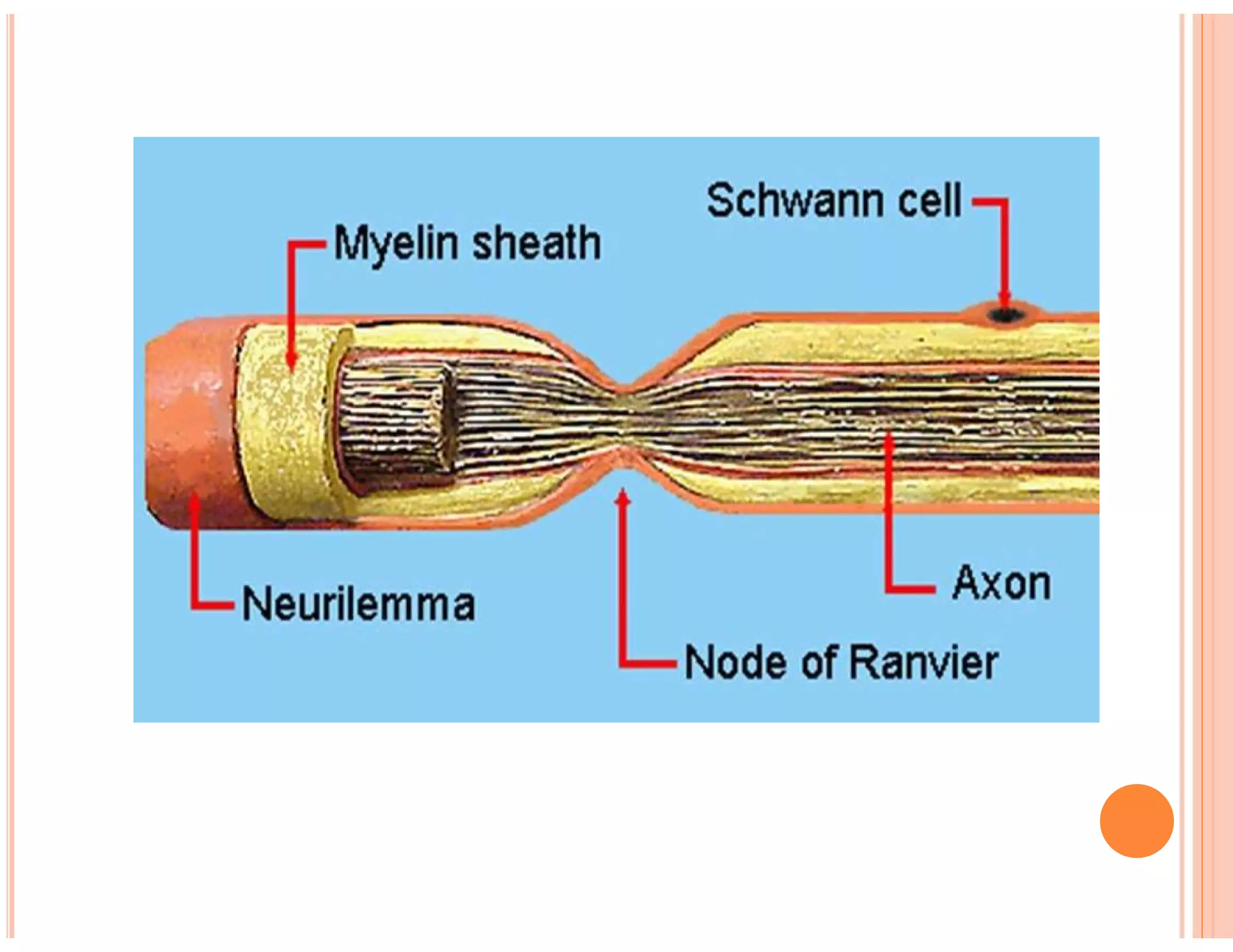
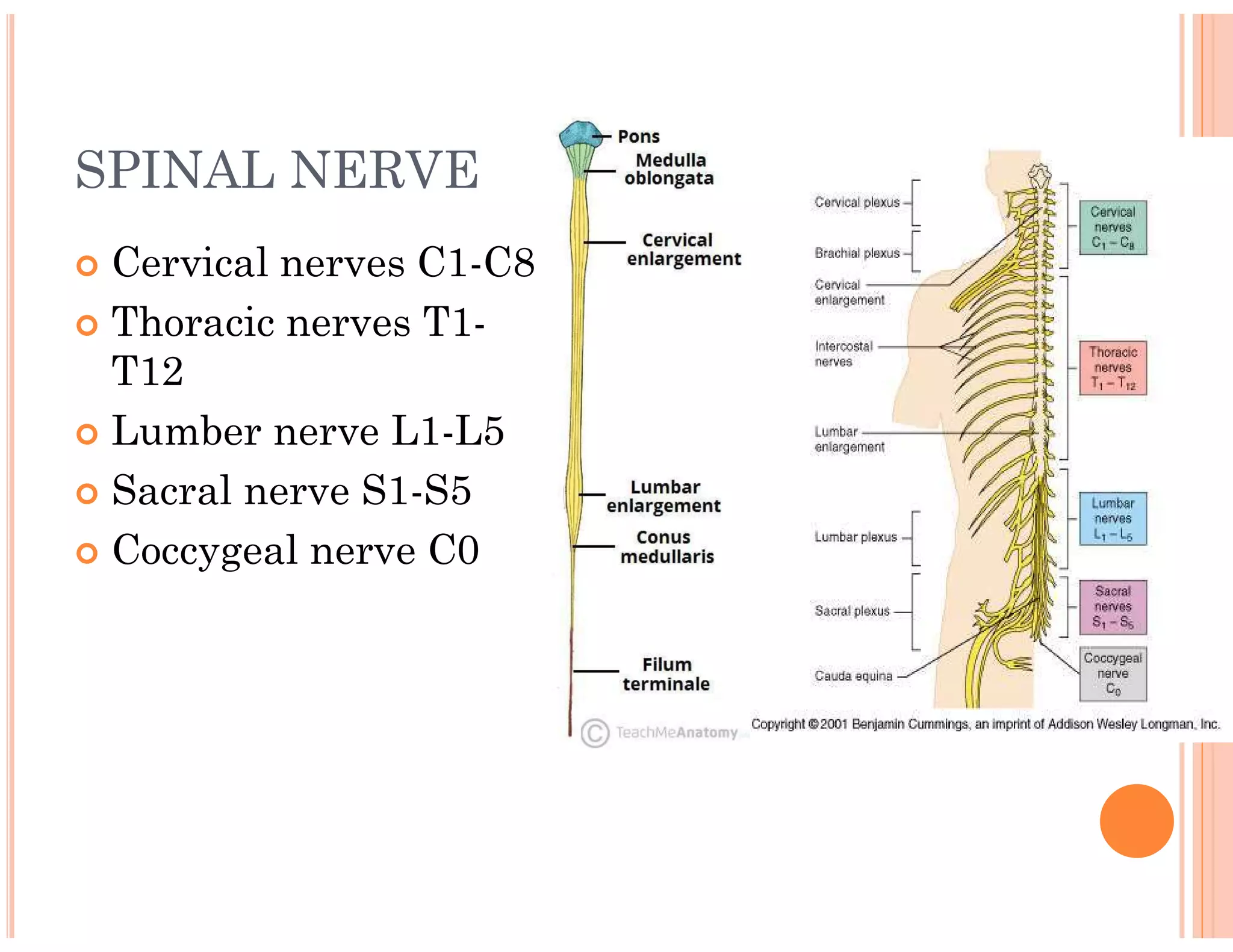
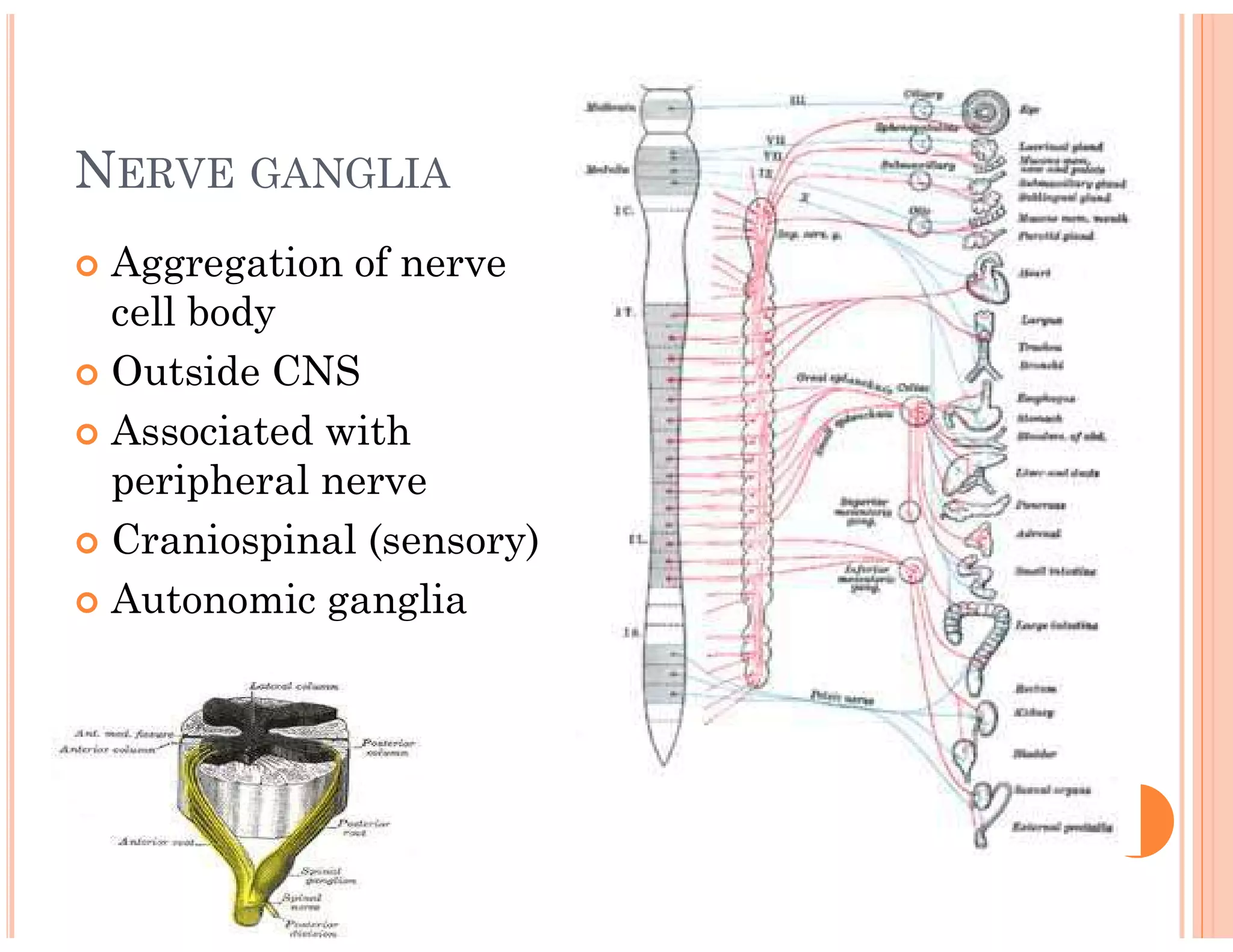
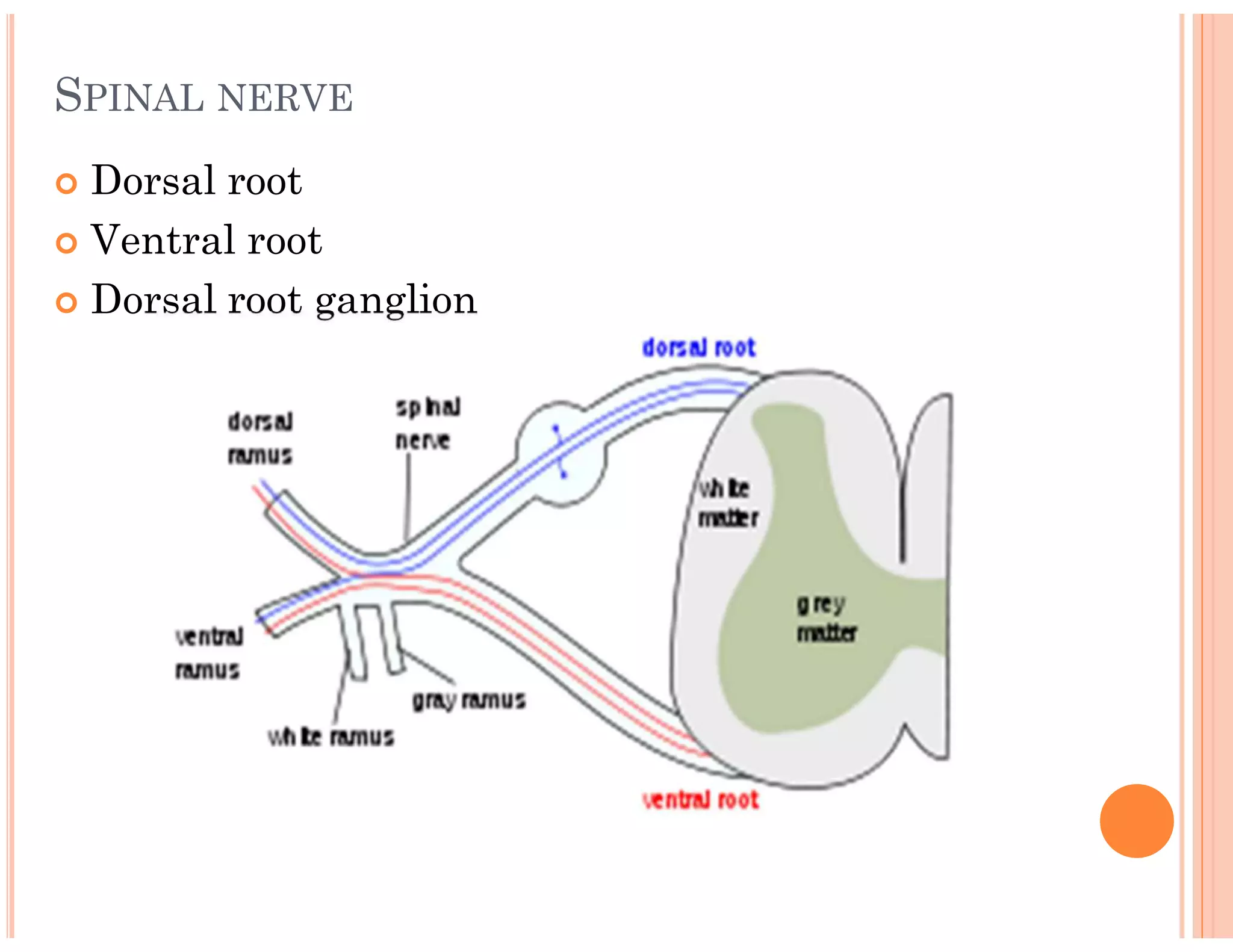
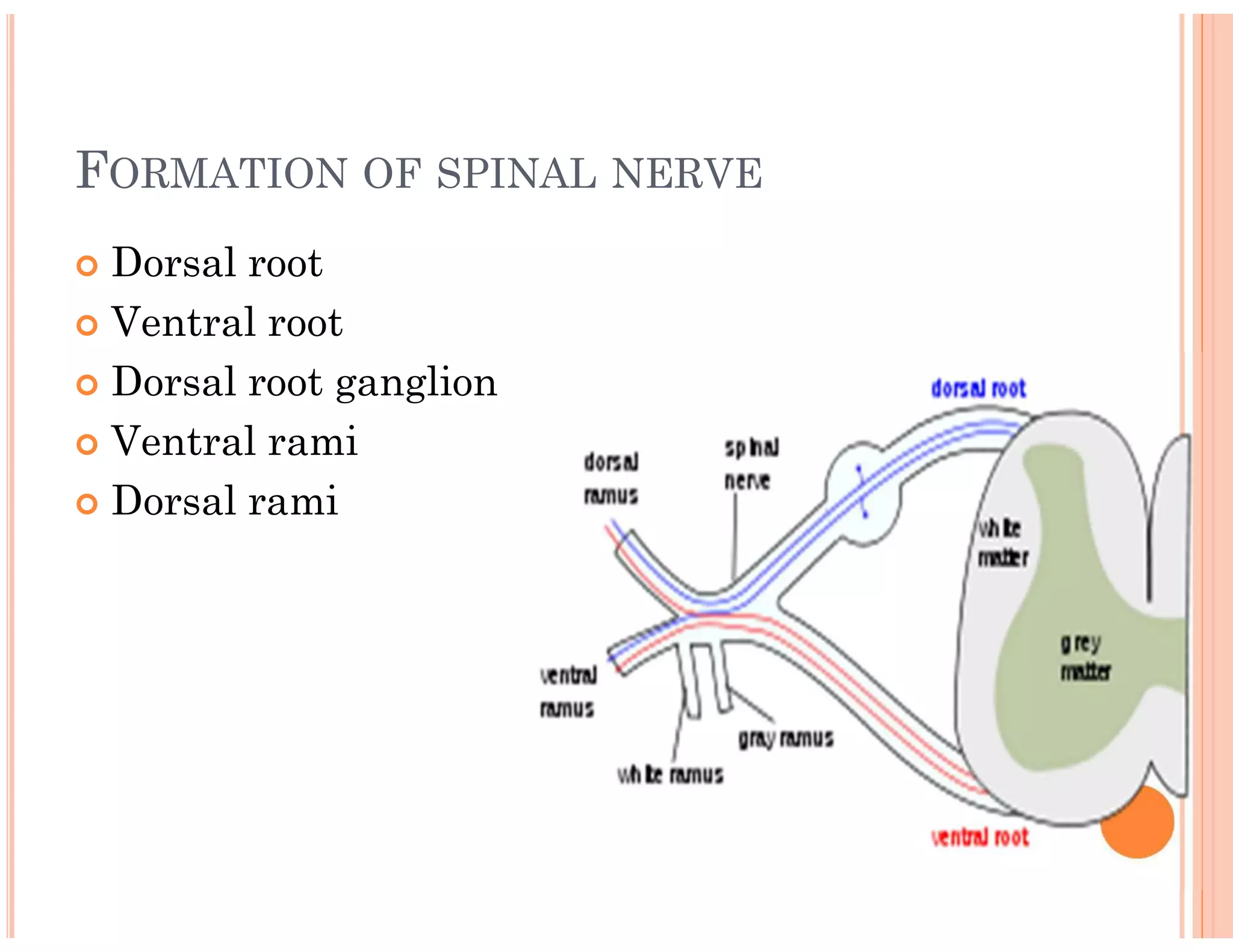
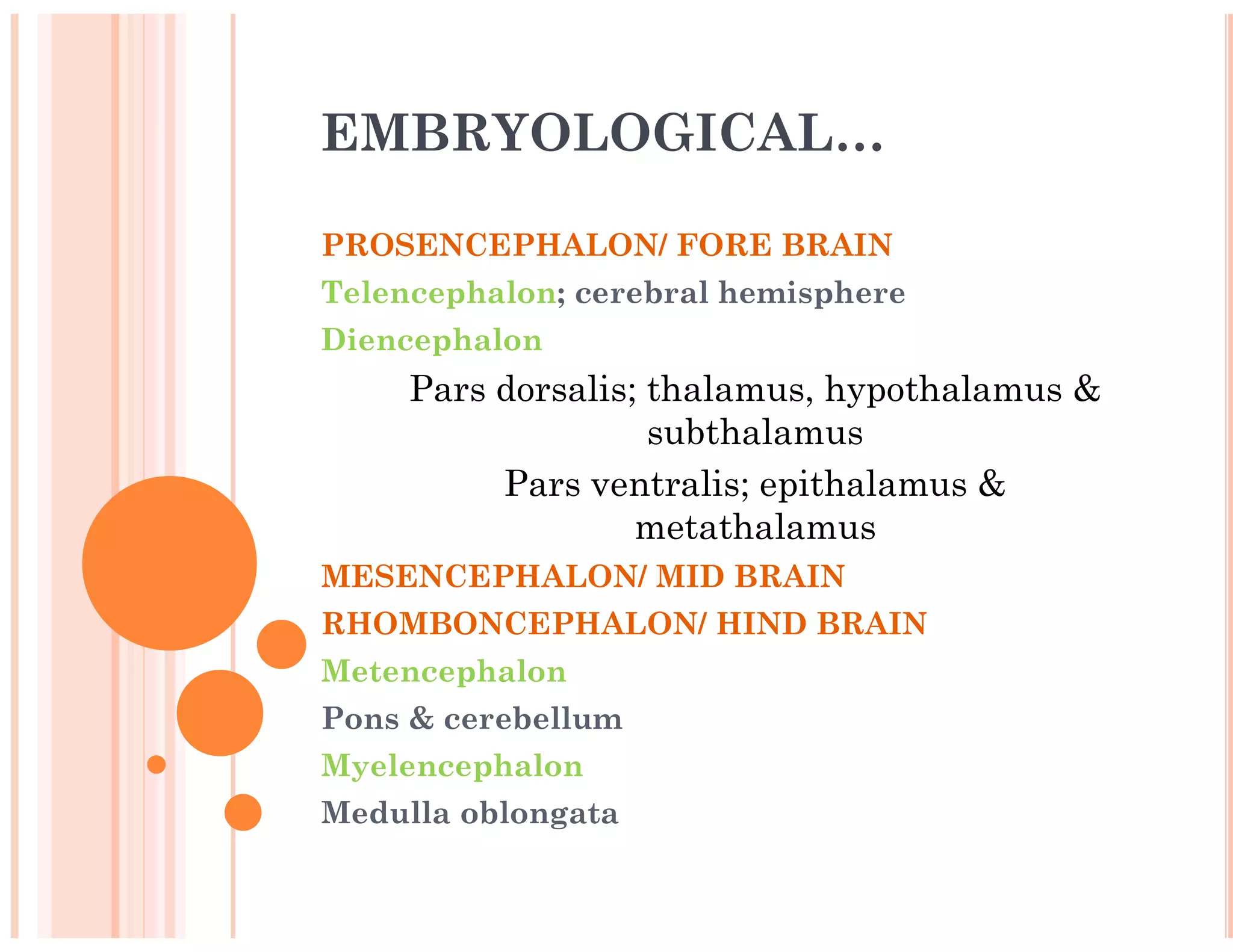
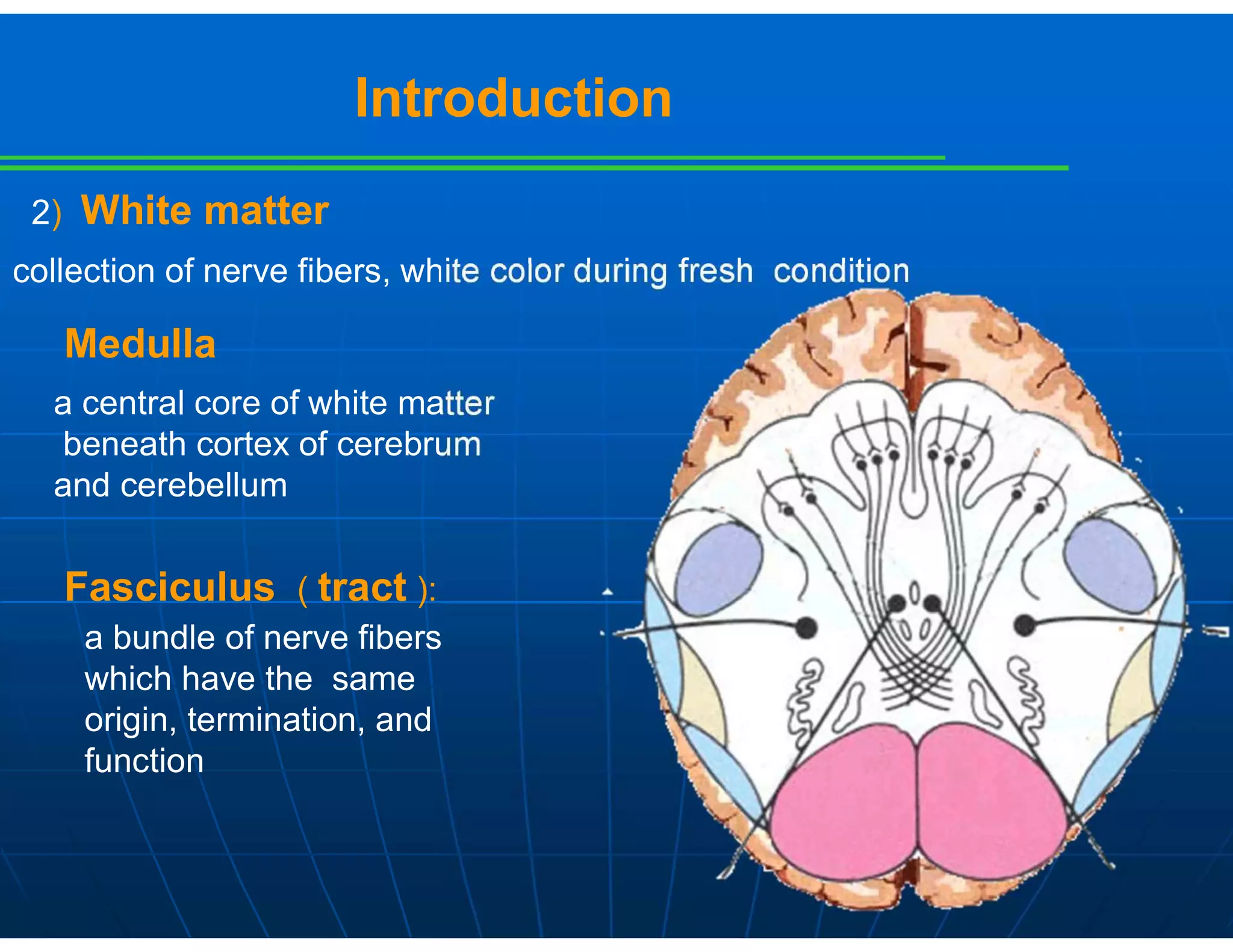
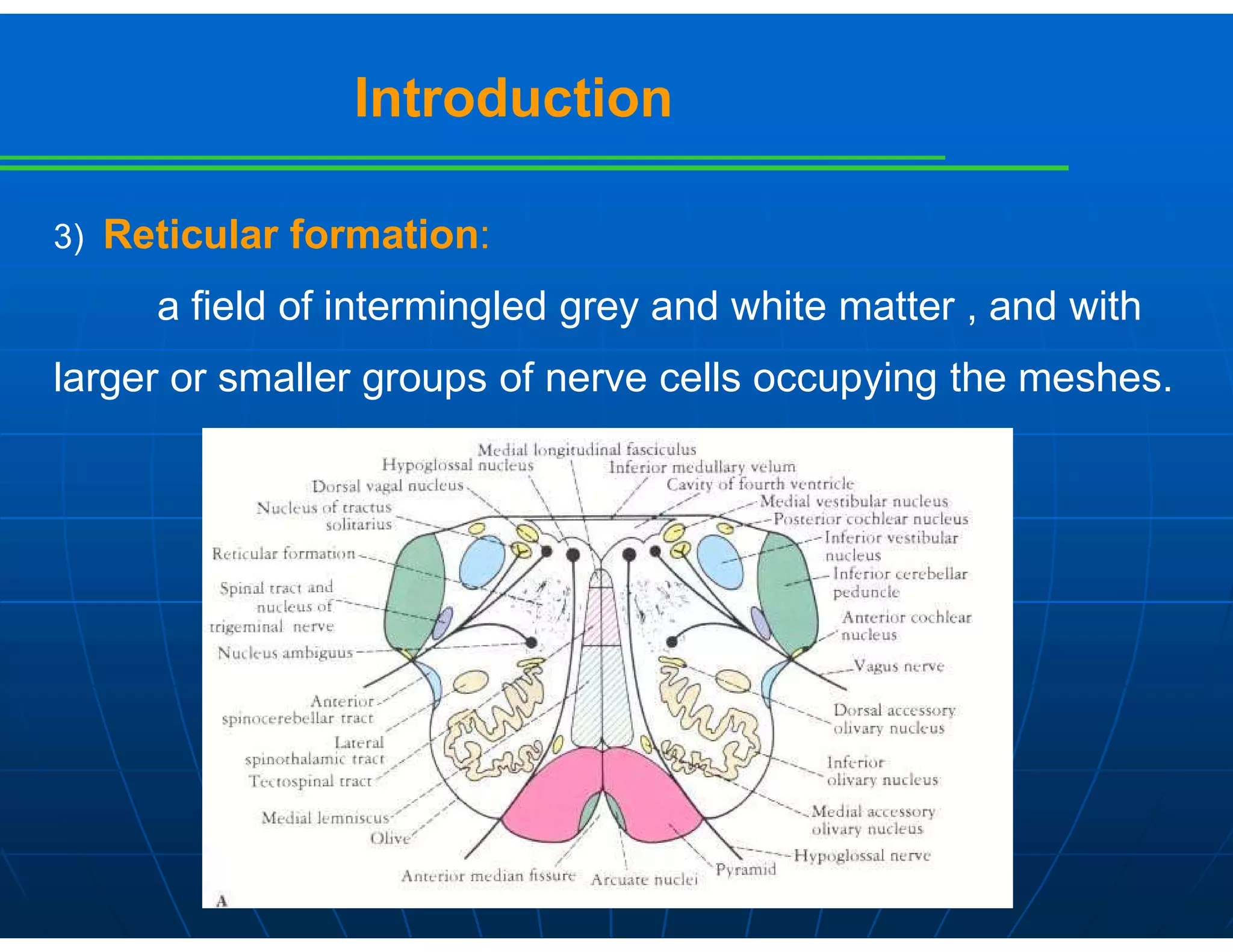
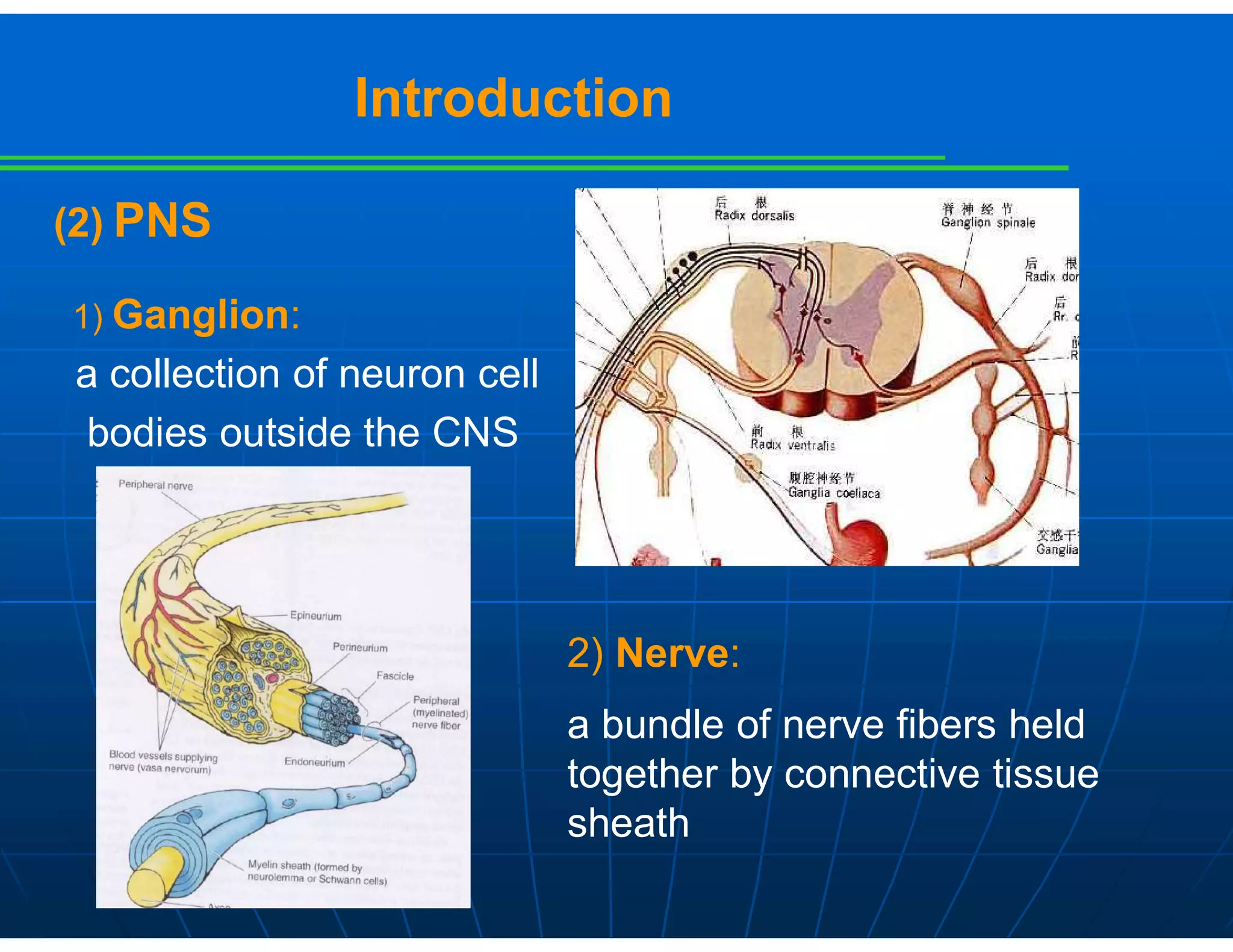
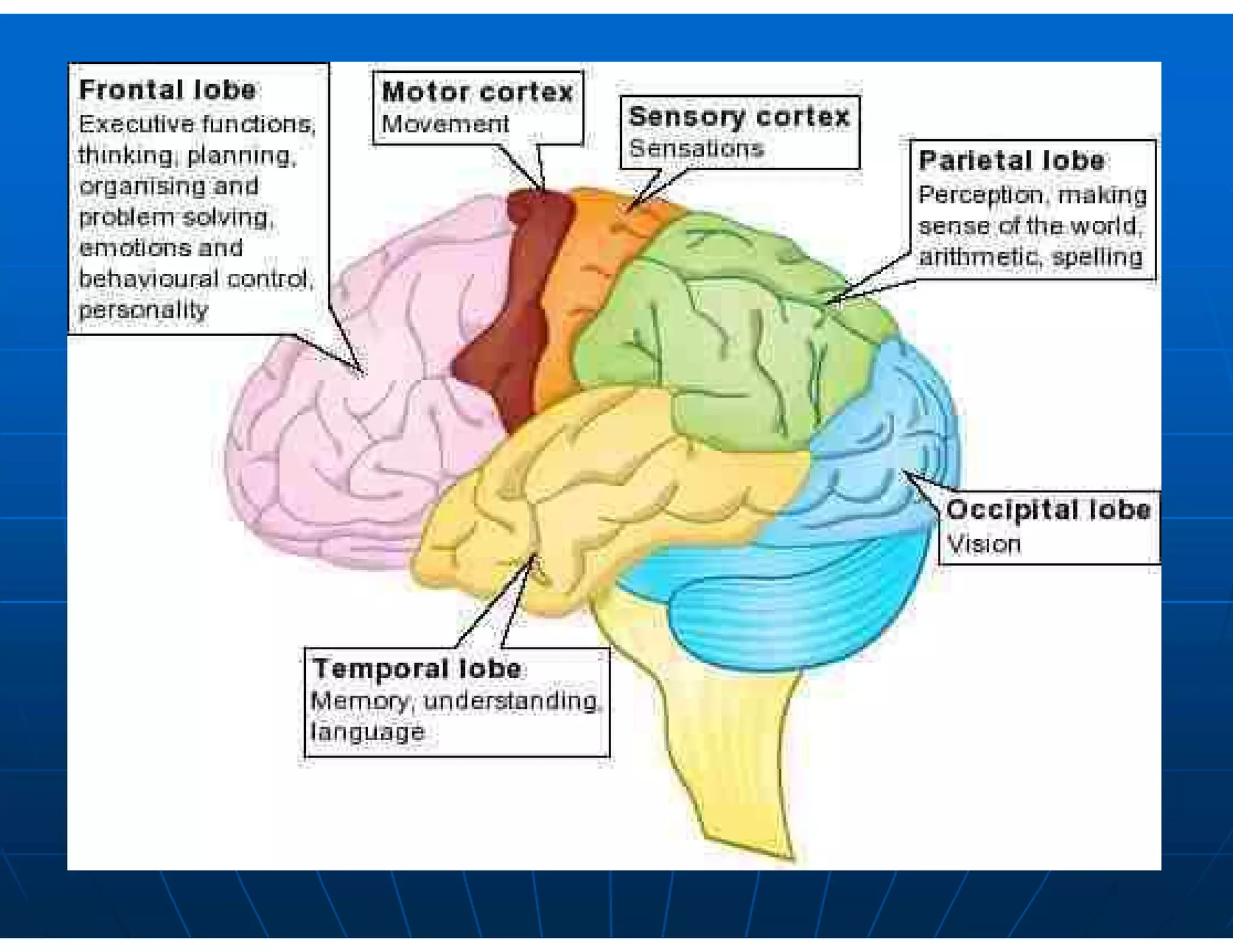
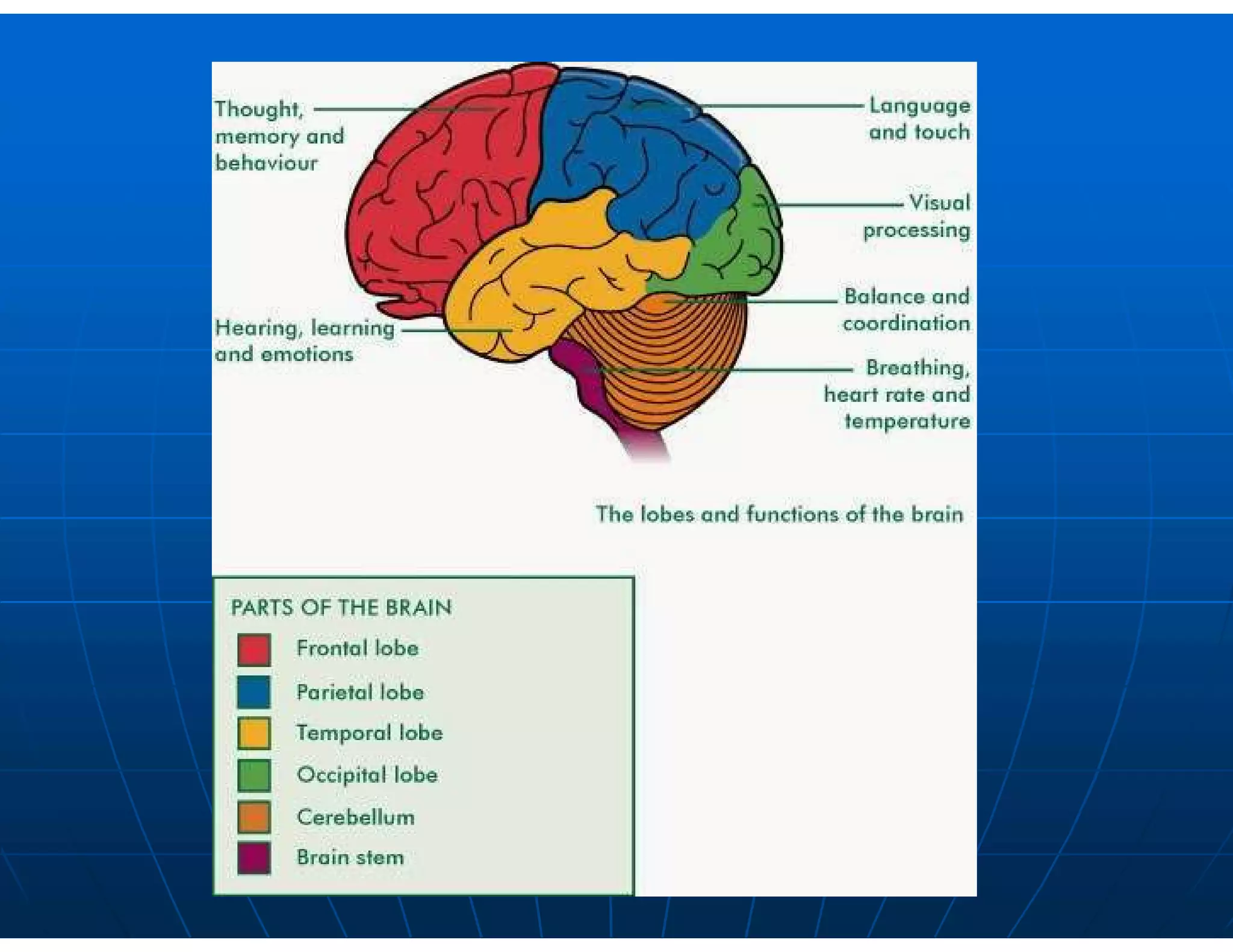
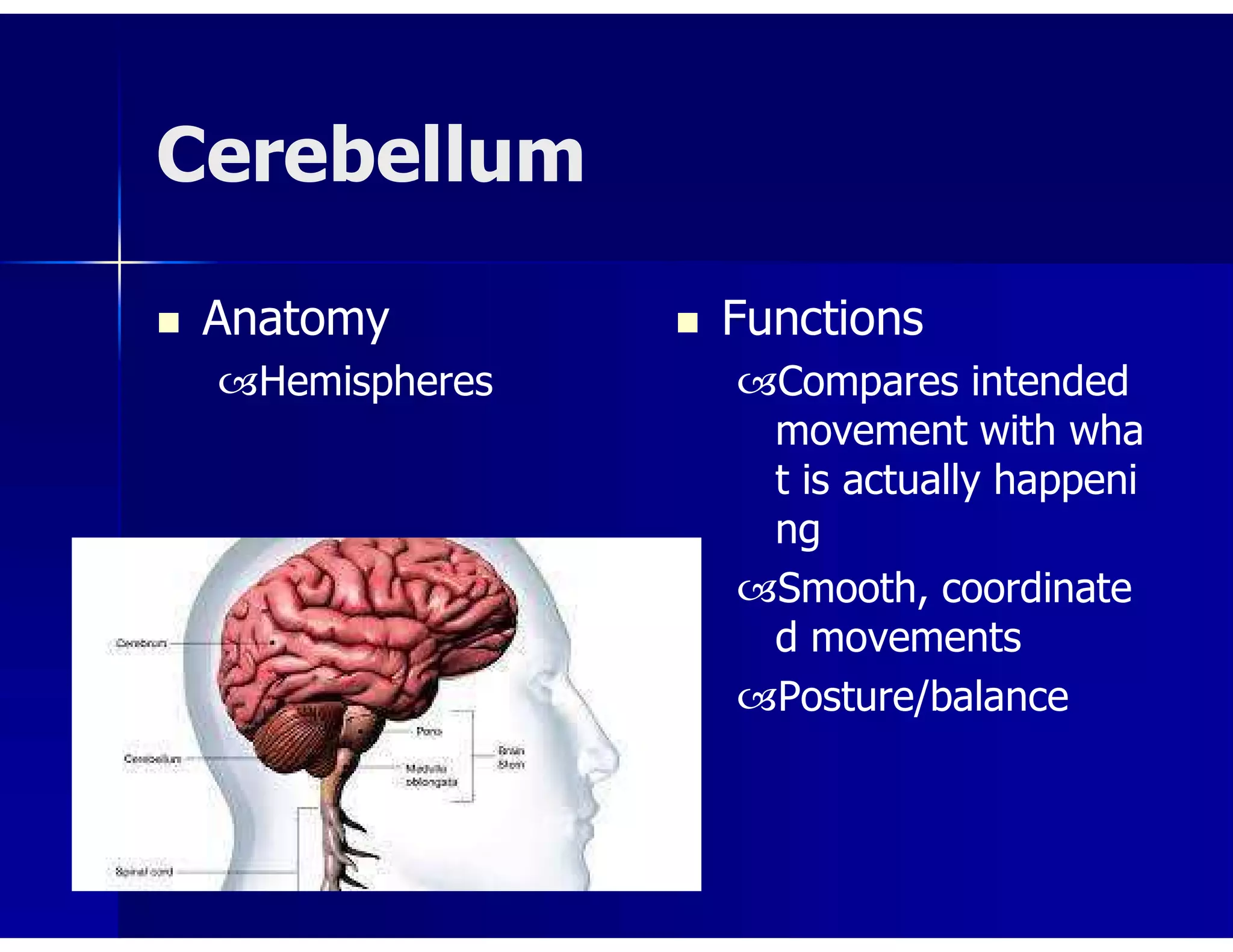
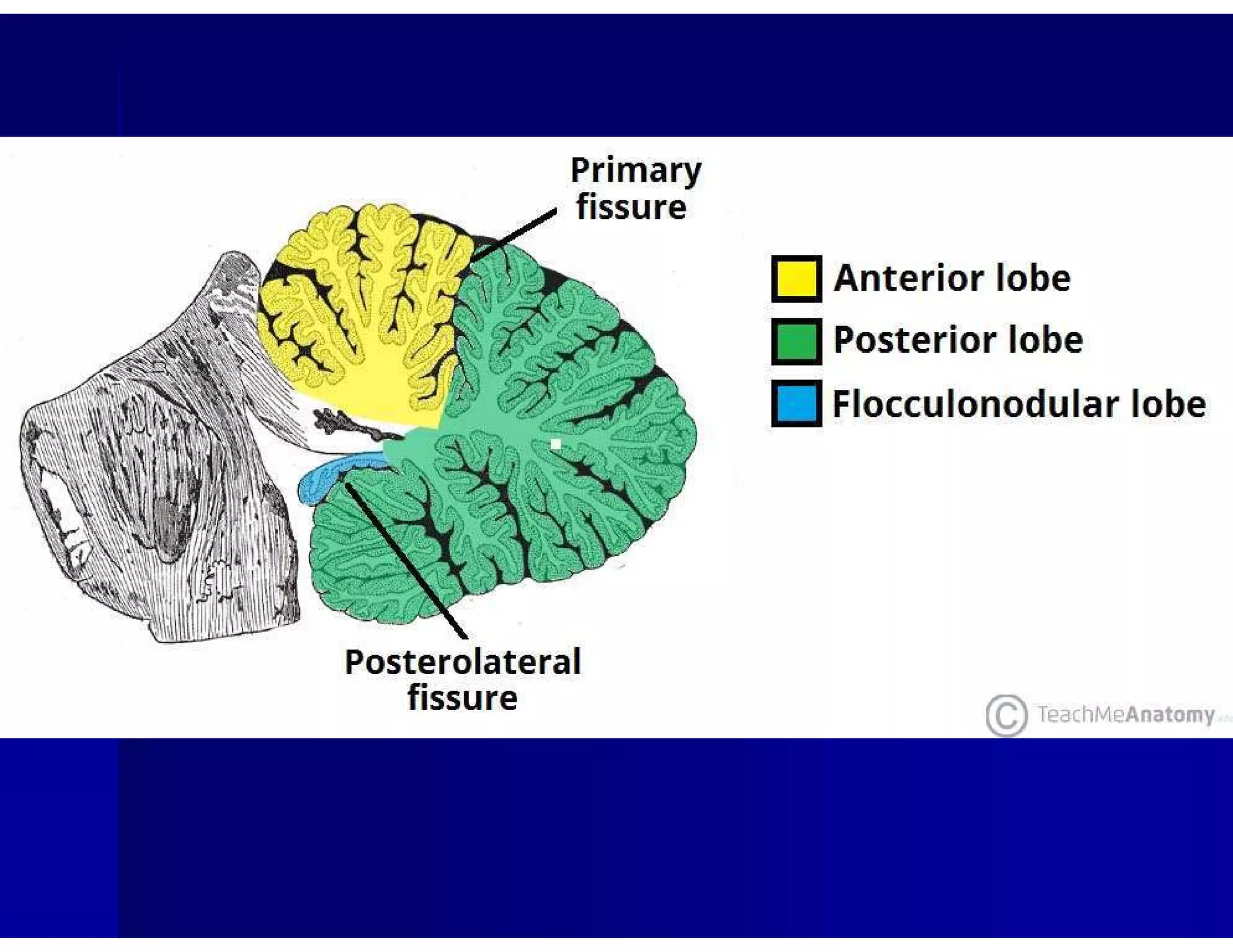
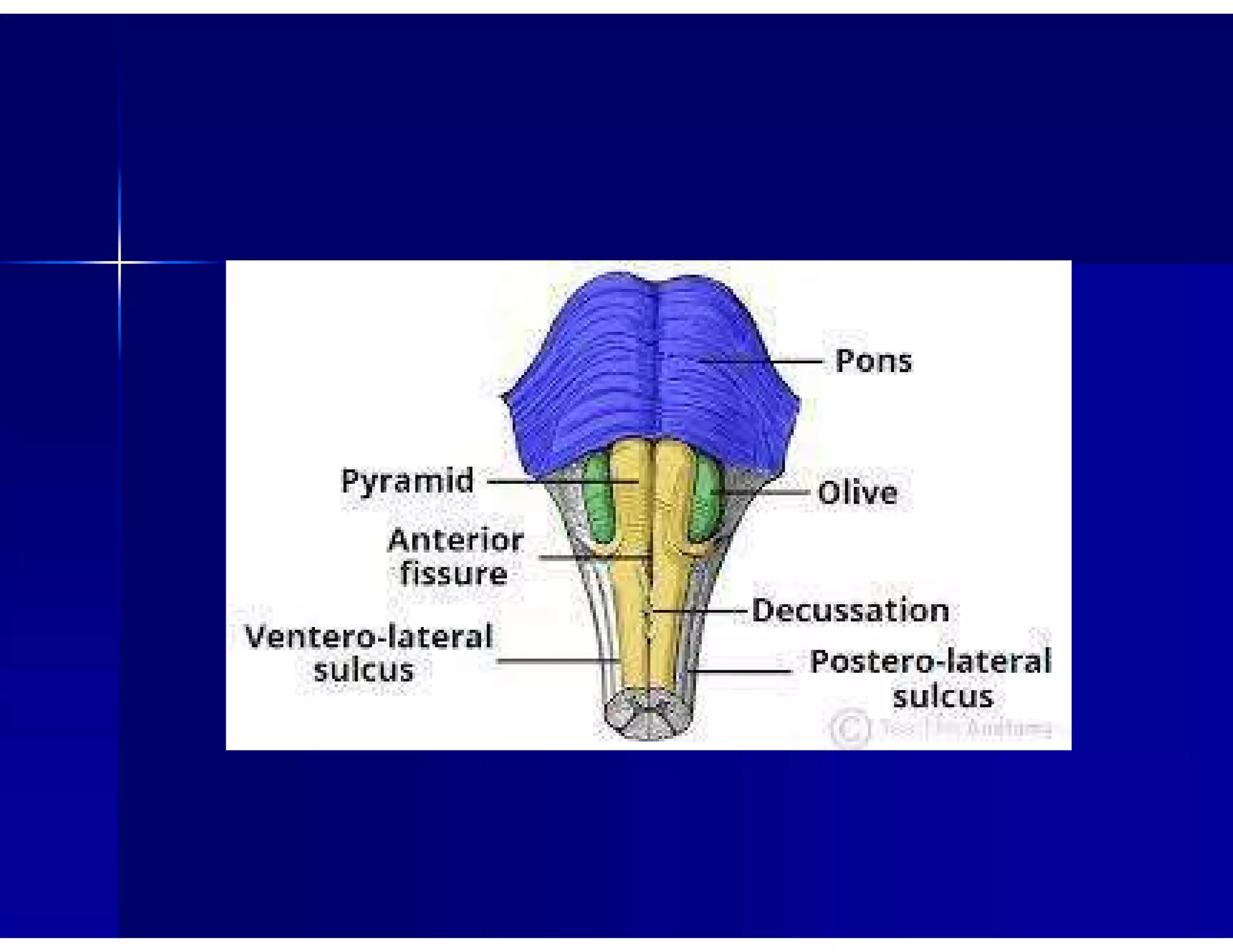
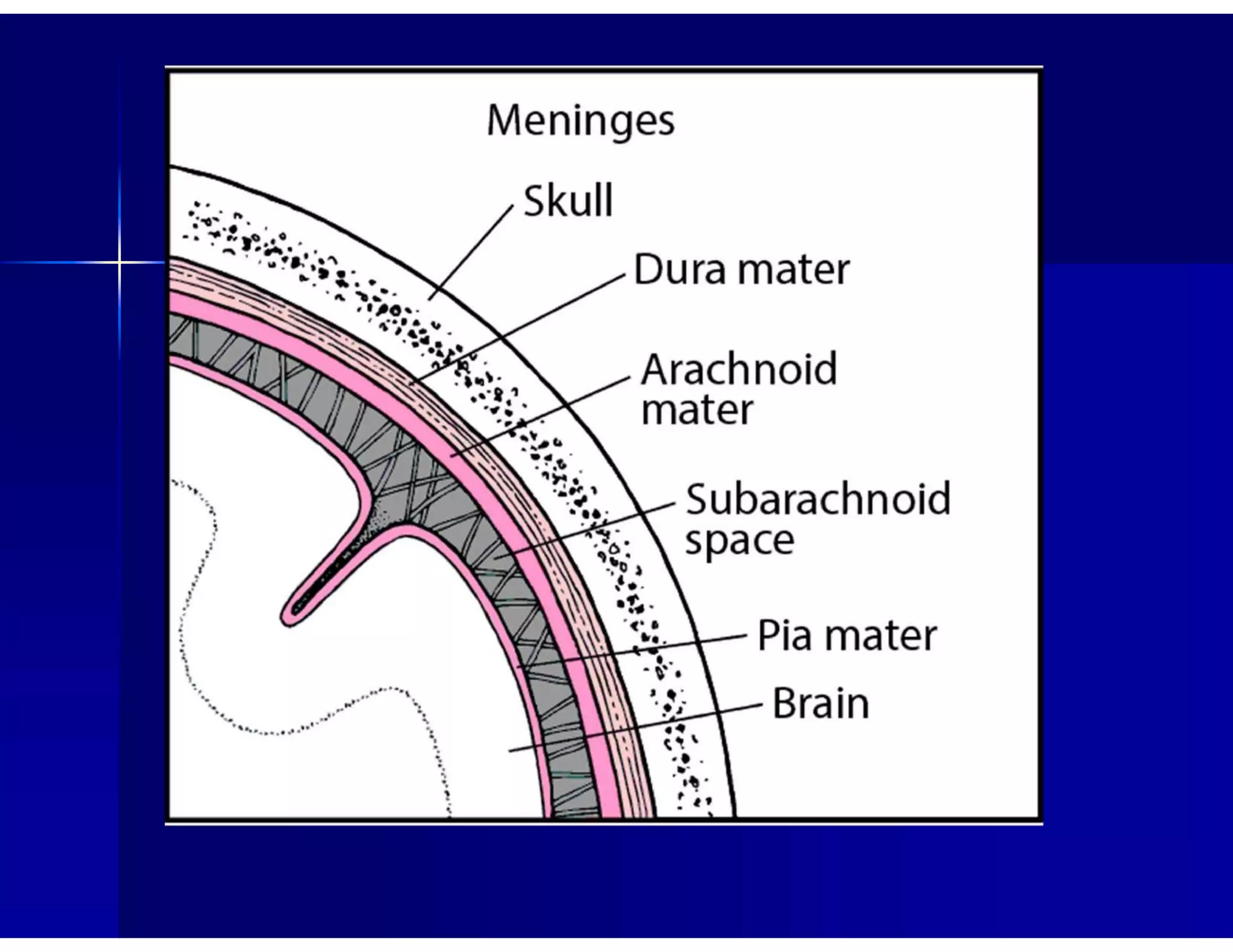
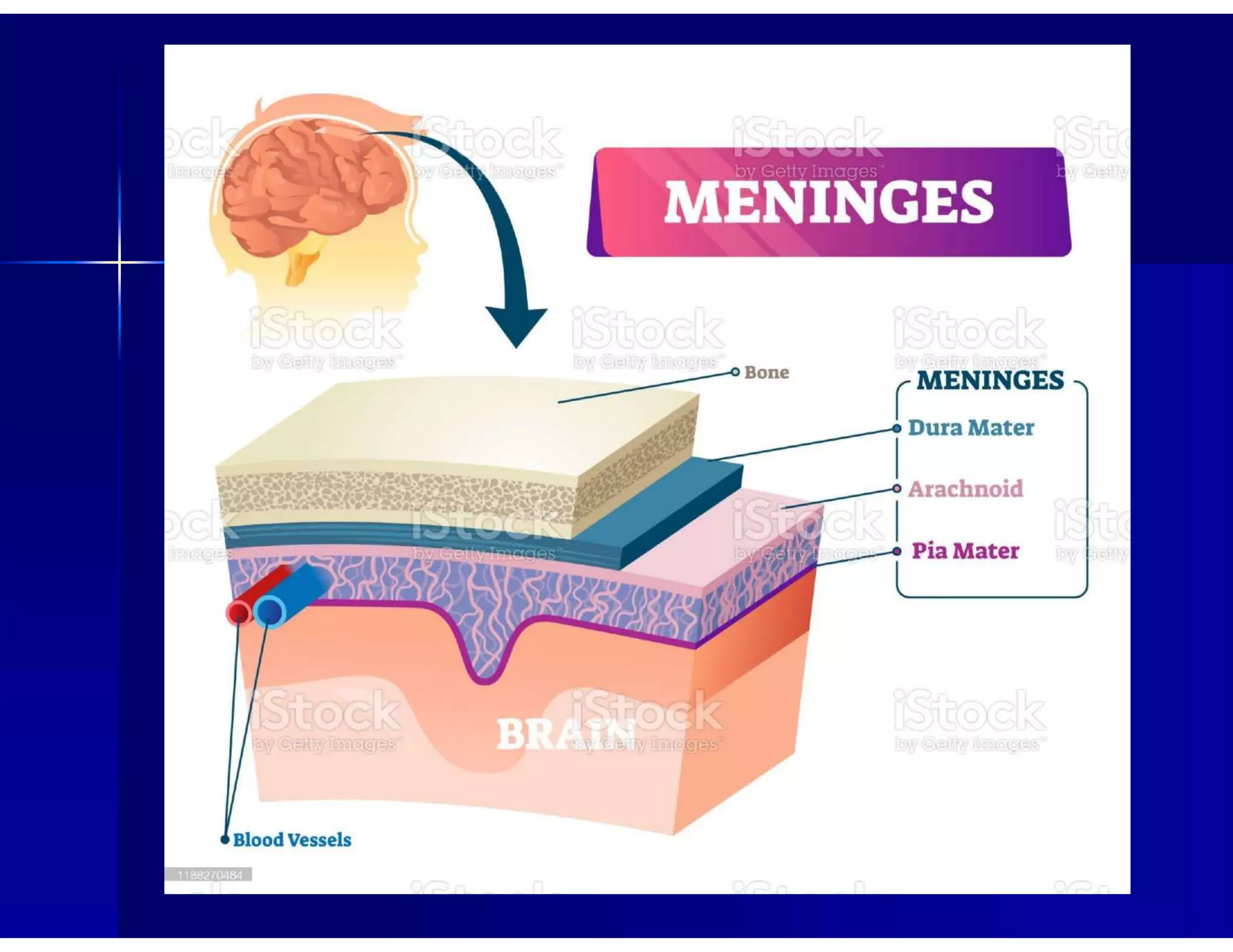
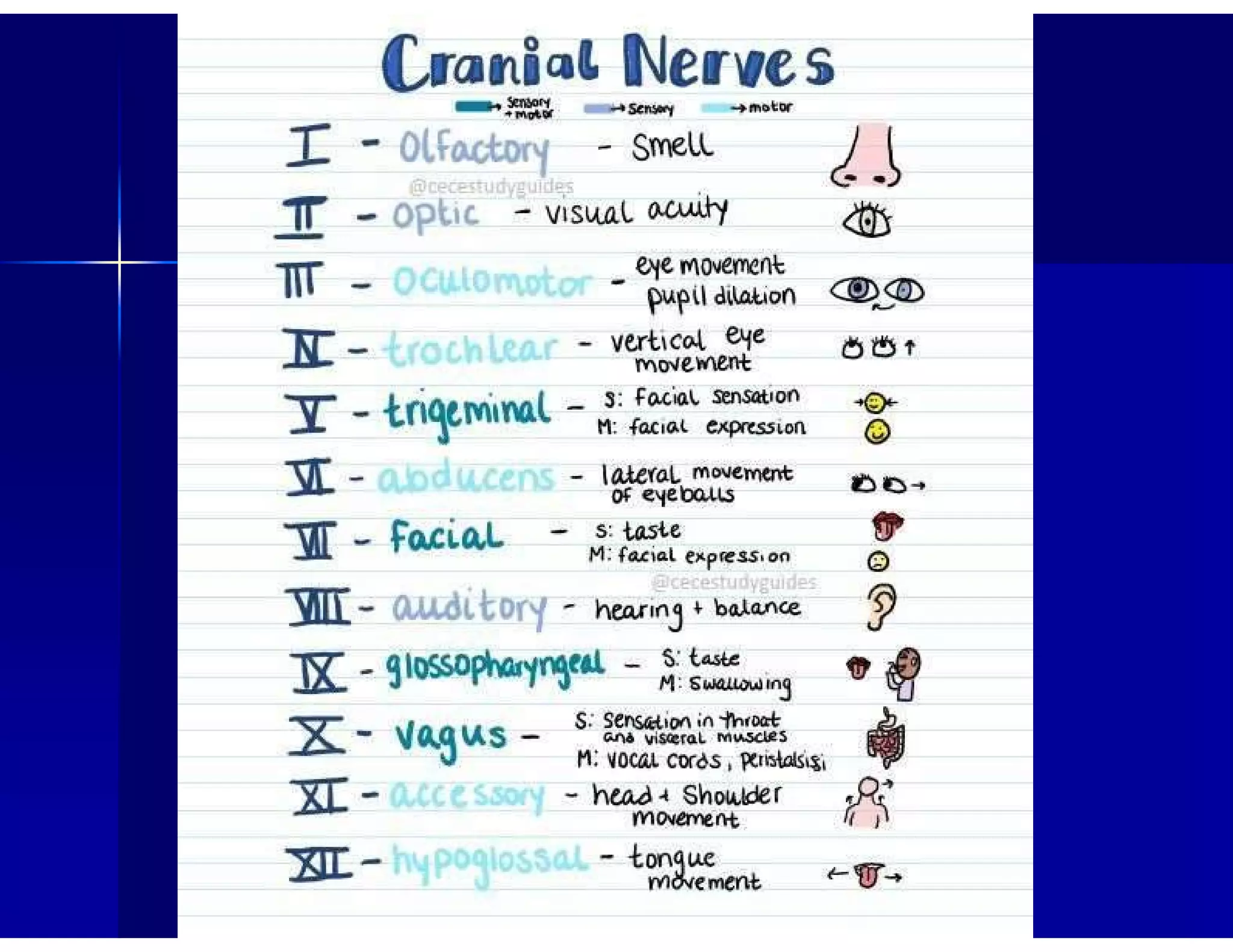
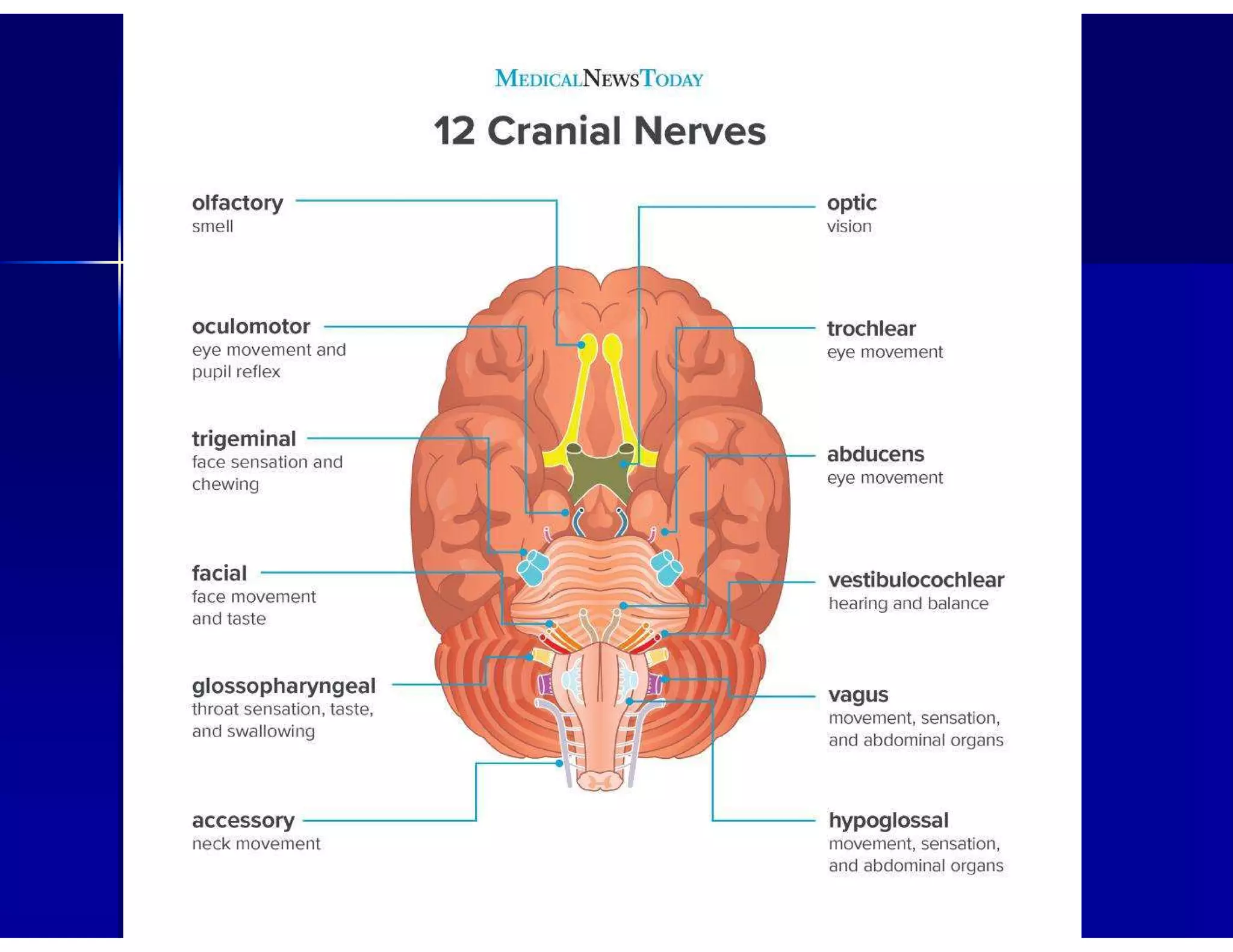
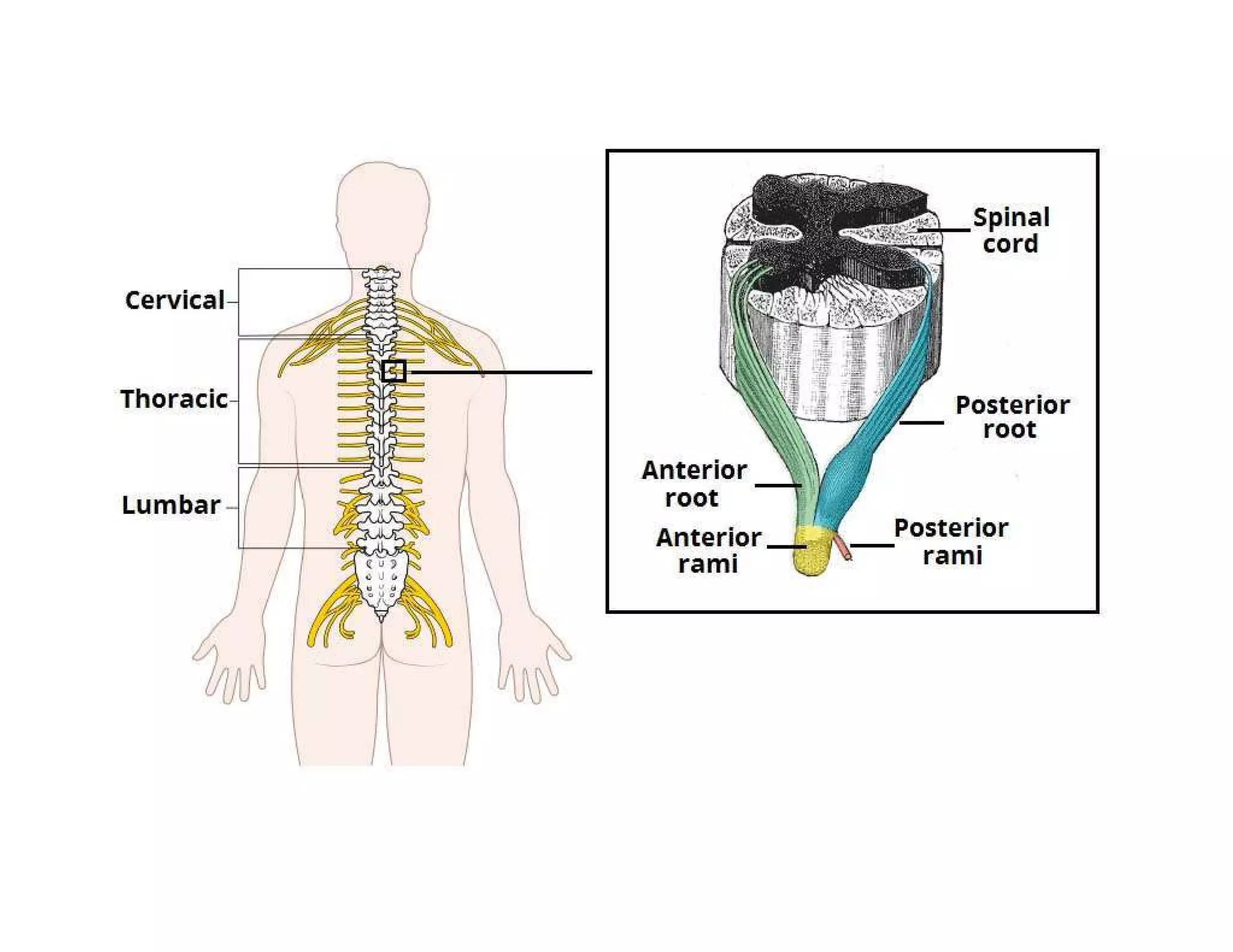
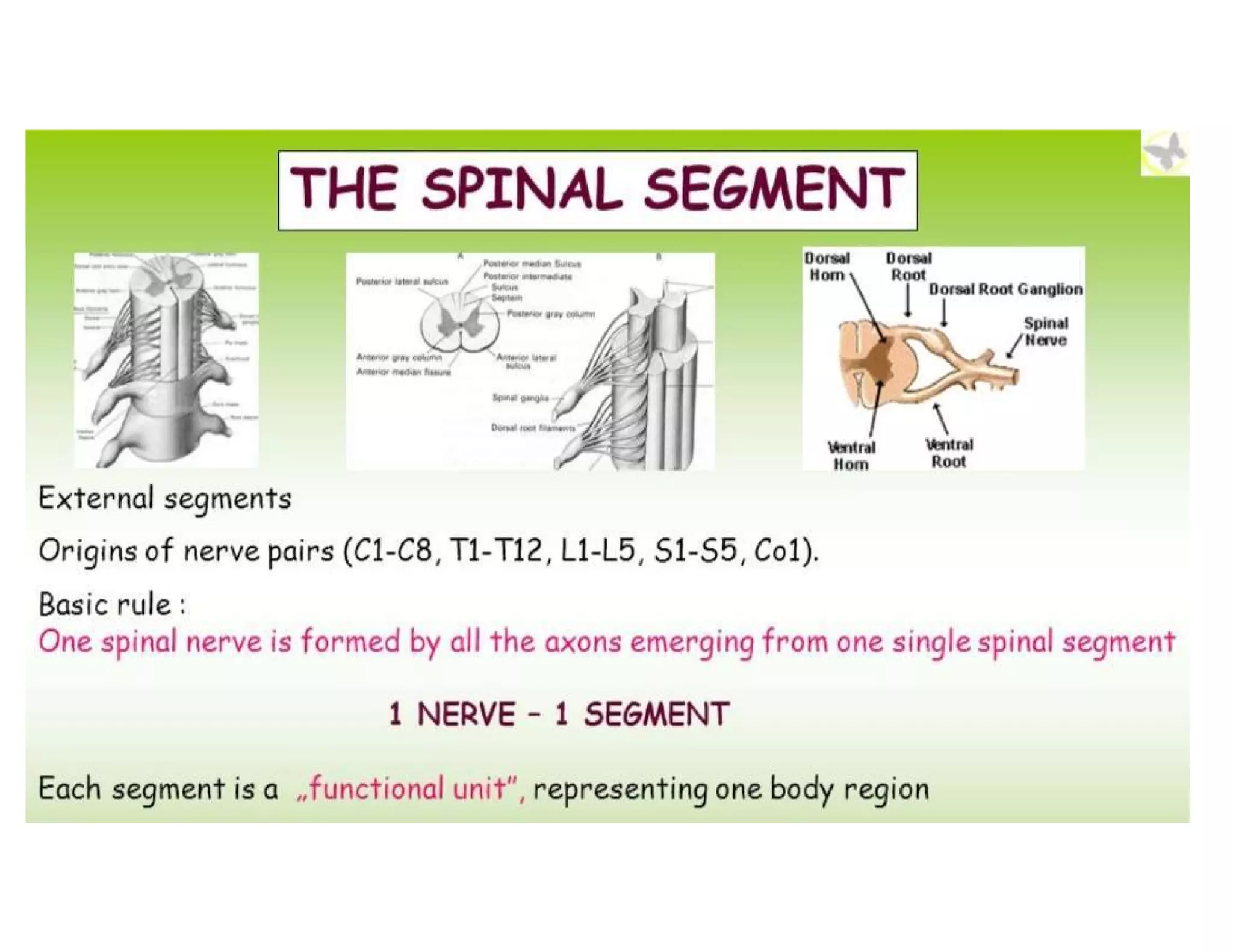
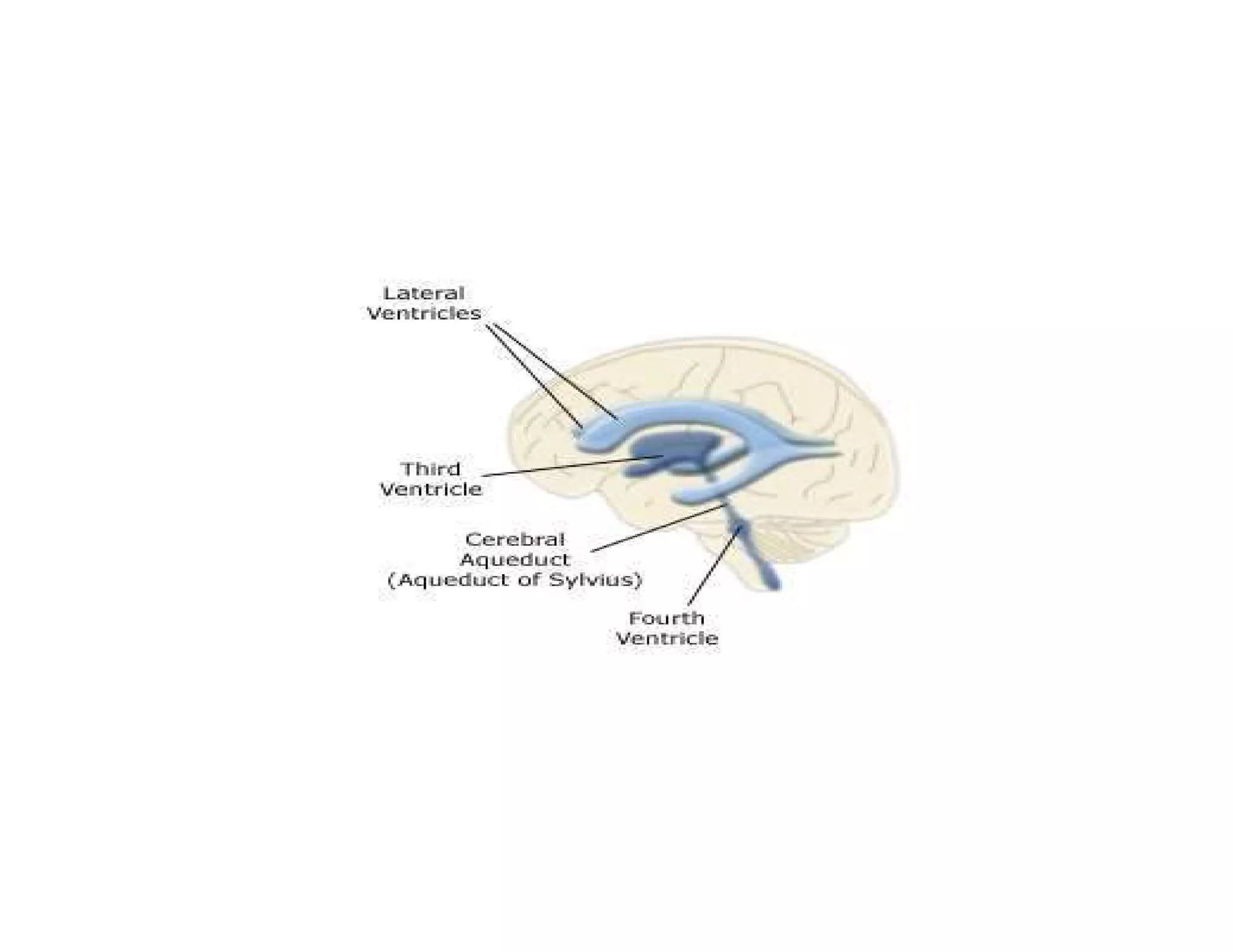
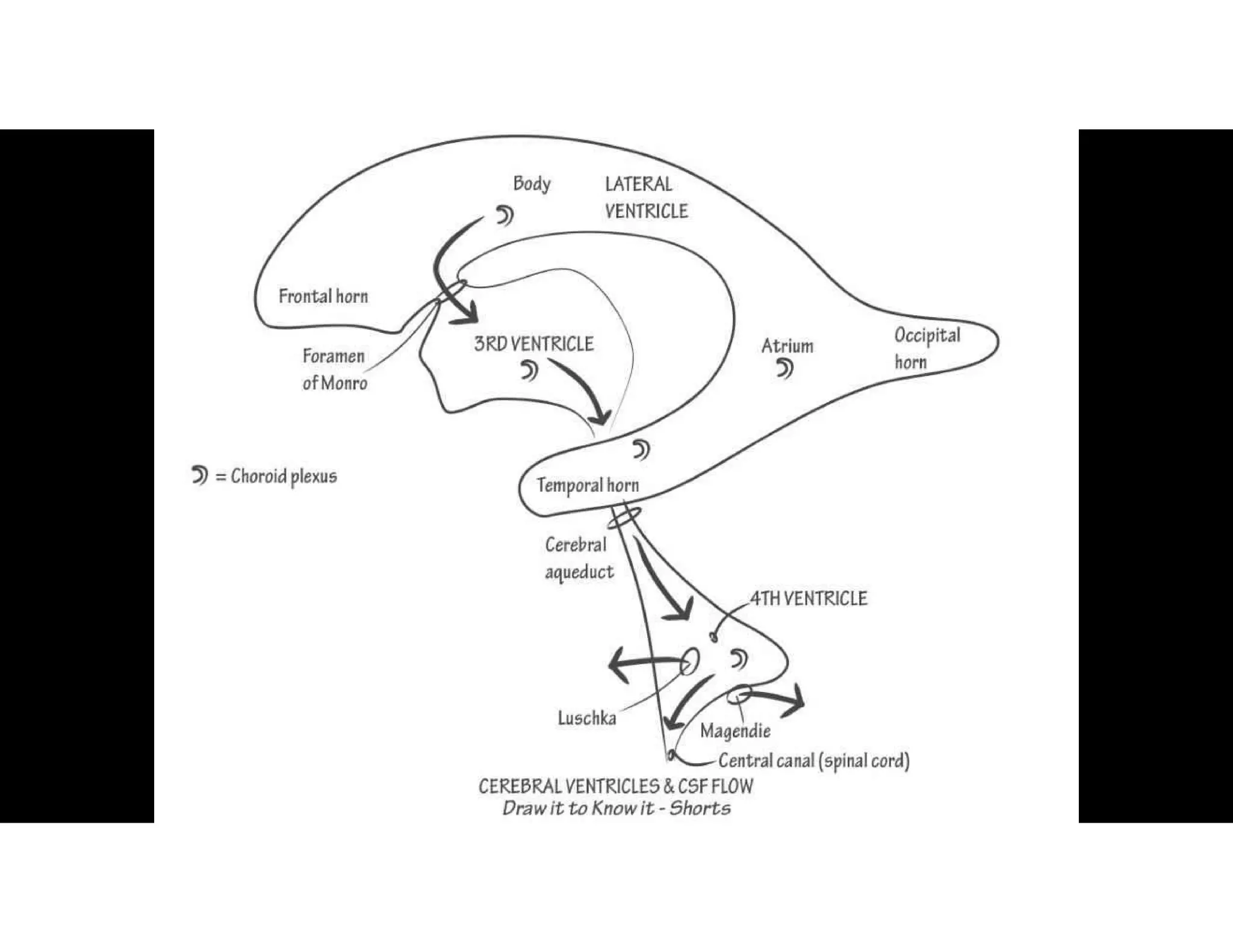
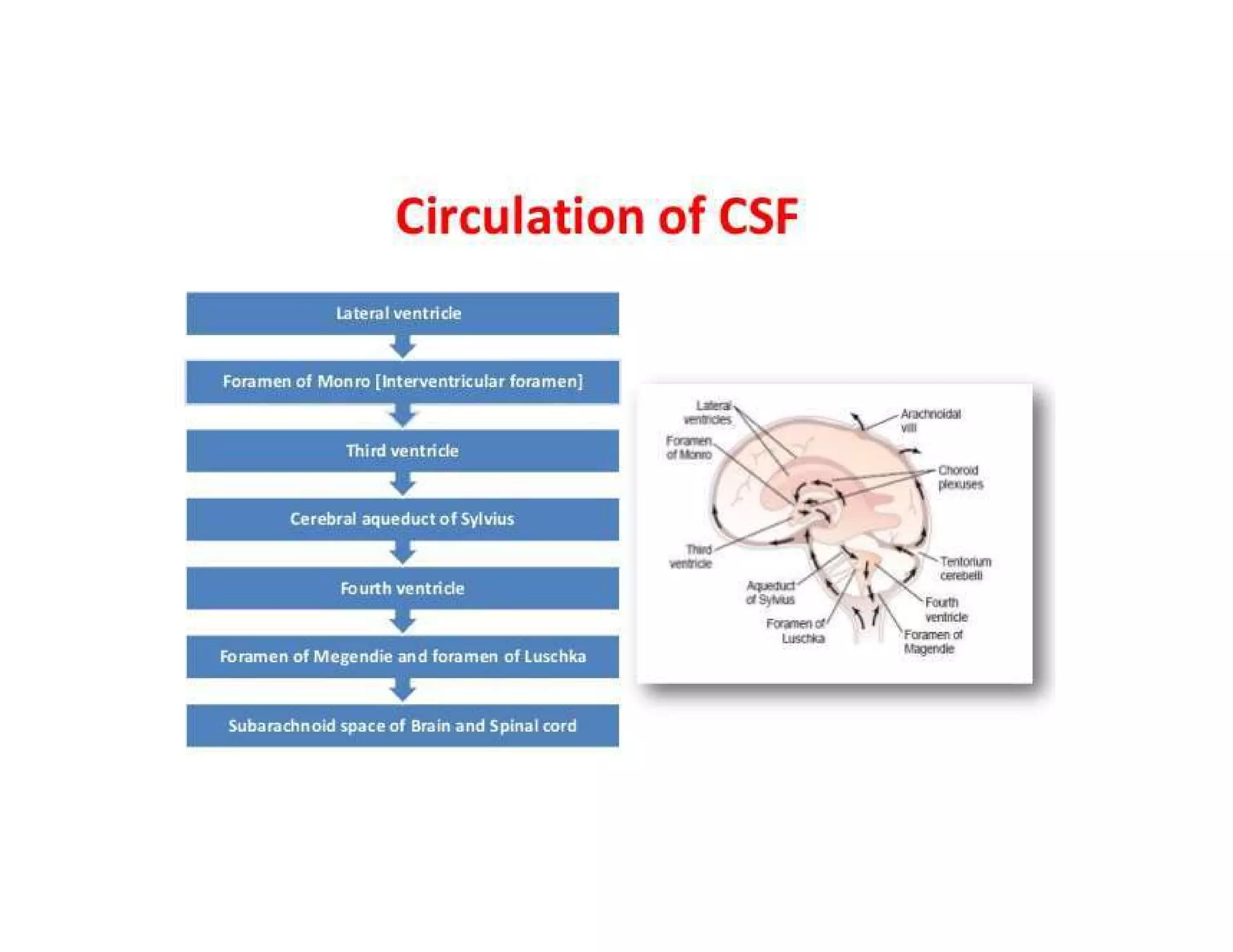
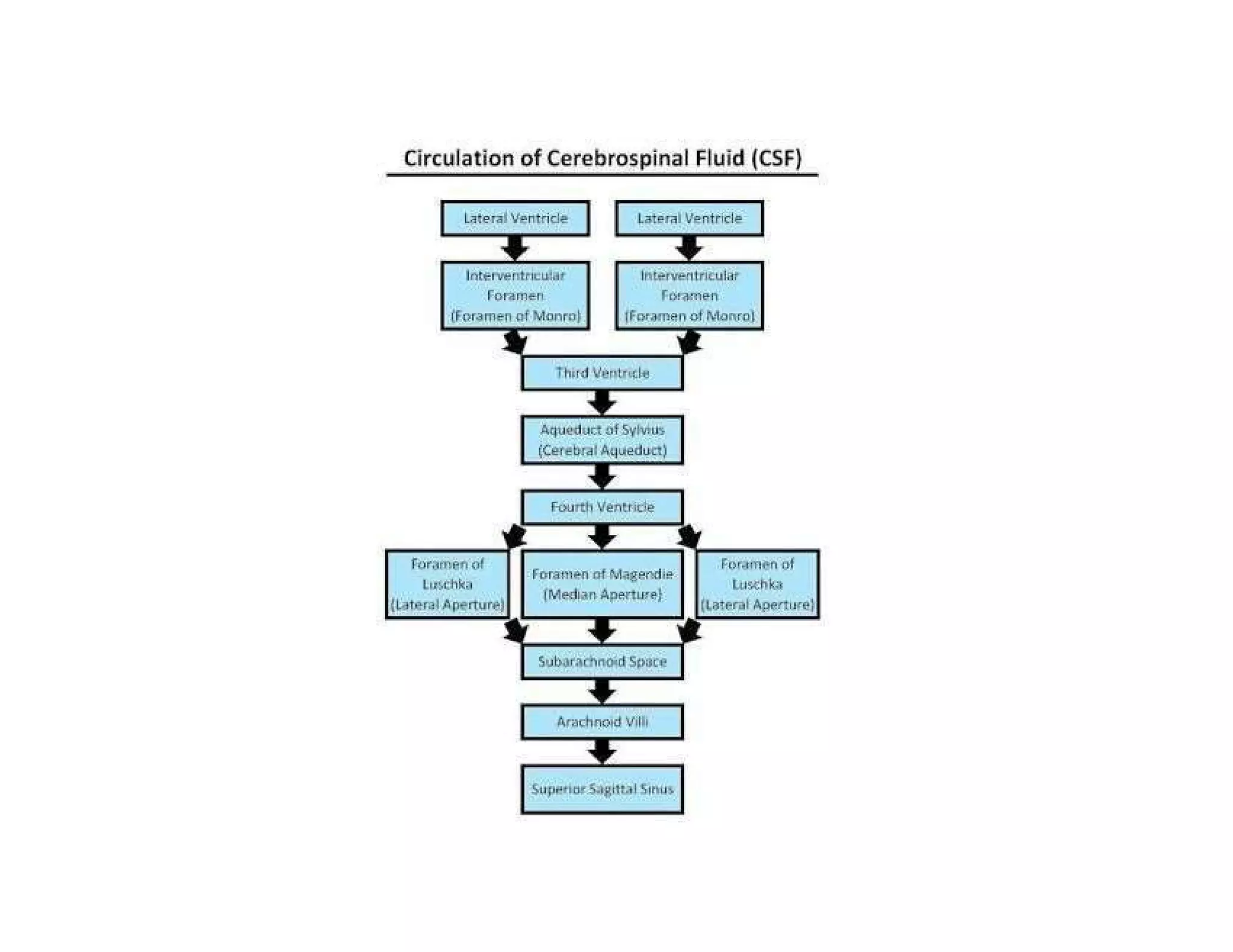
Explains the central and peripheral nervous systems, their structure, function, and cellular components.
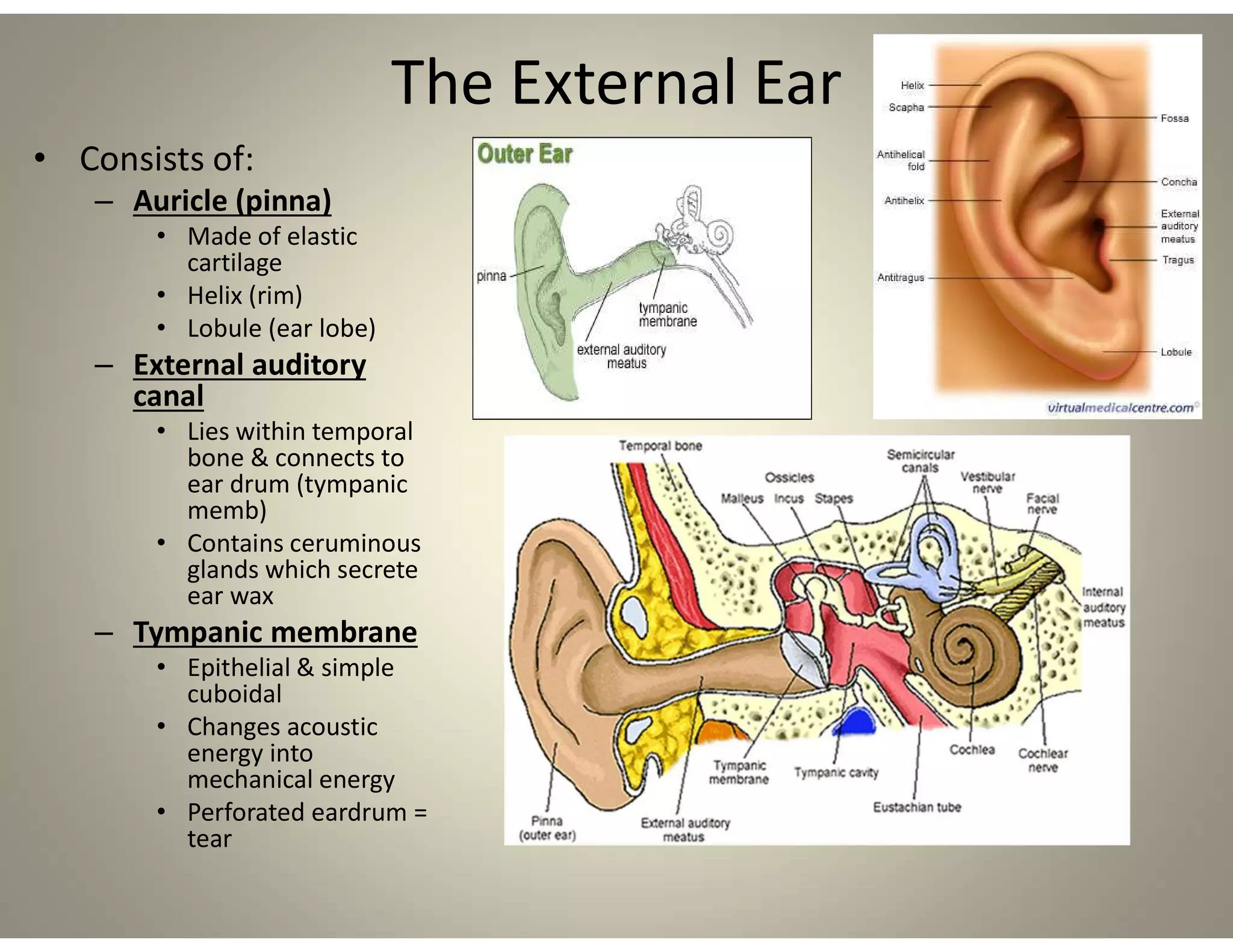
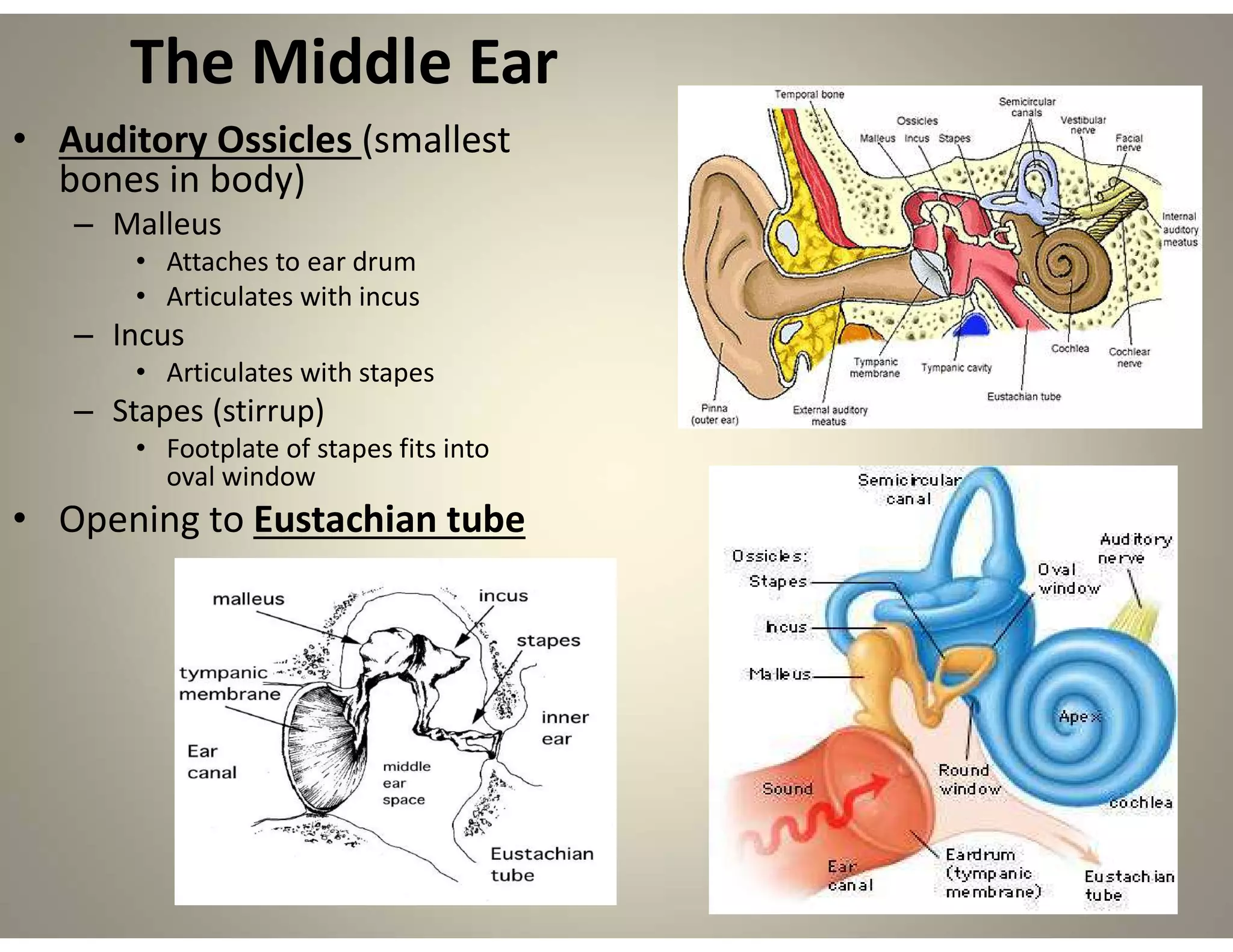
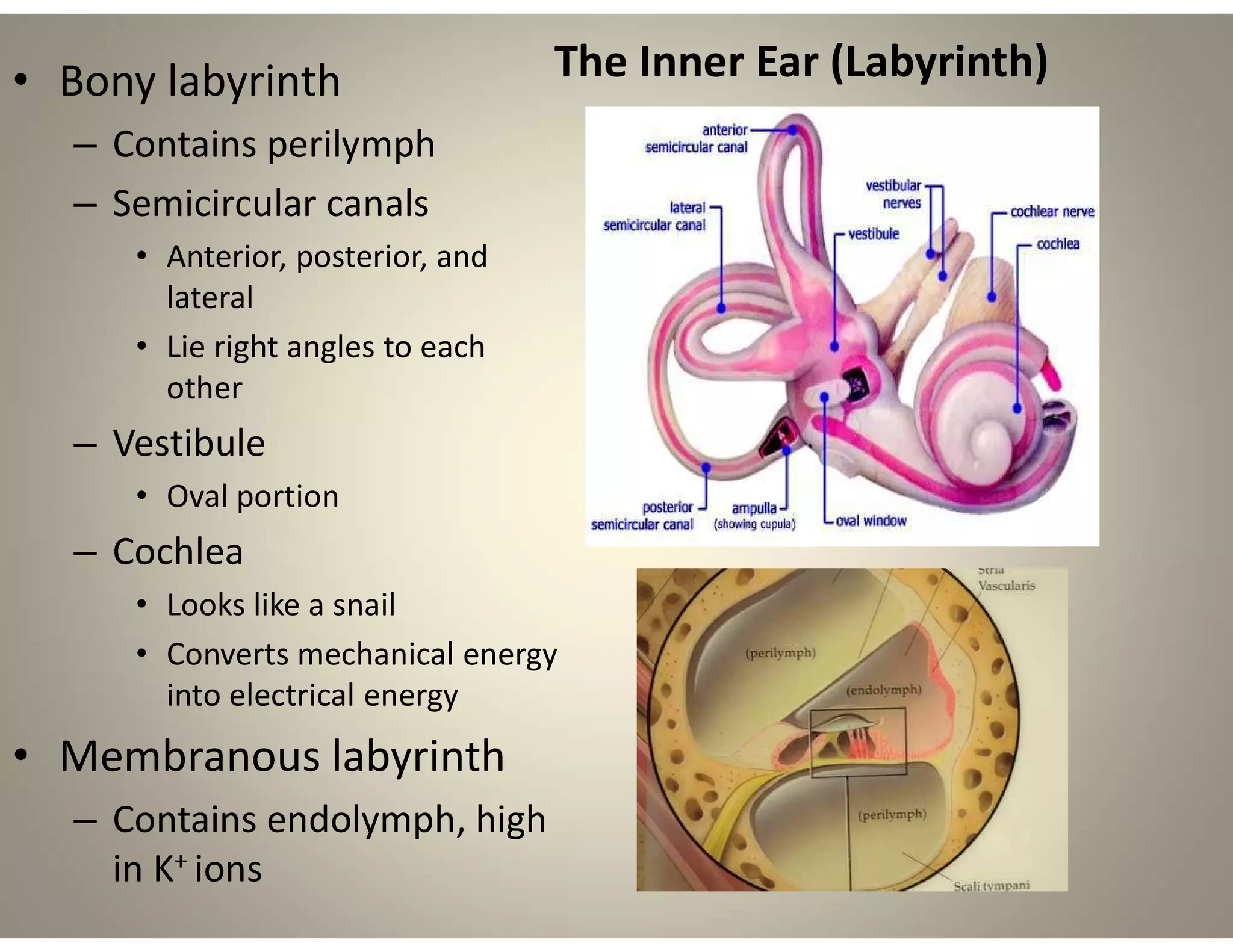
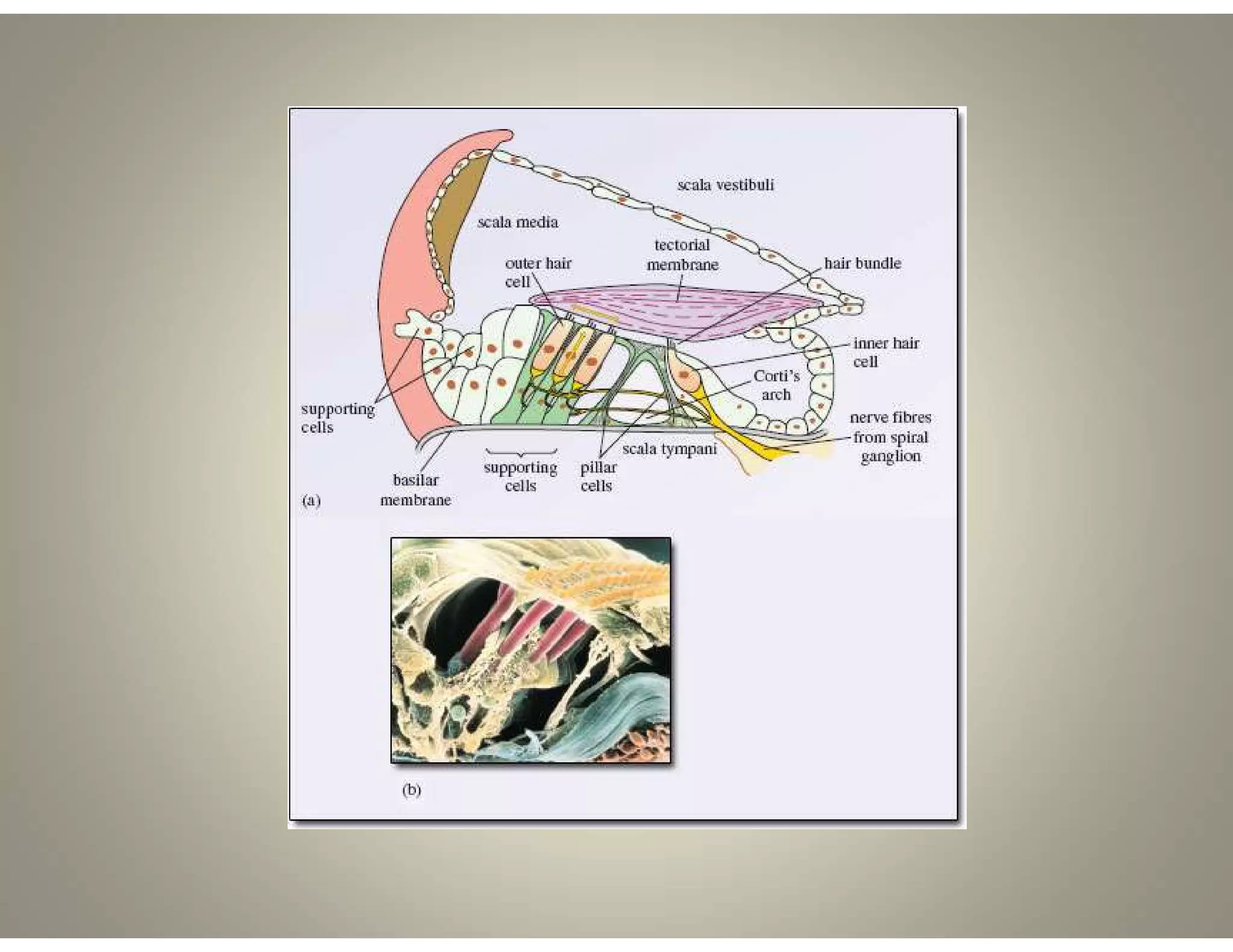
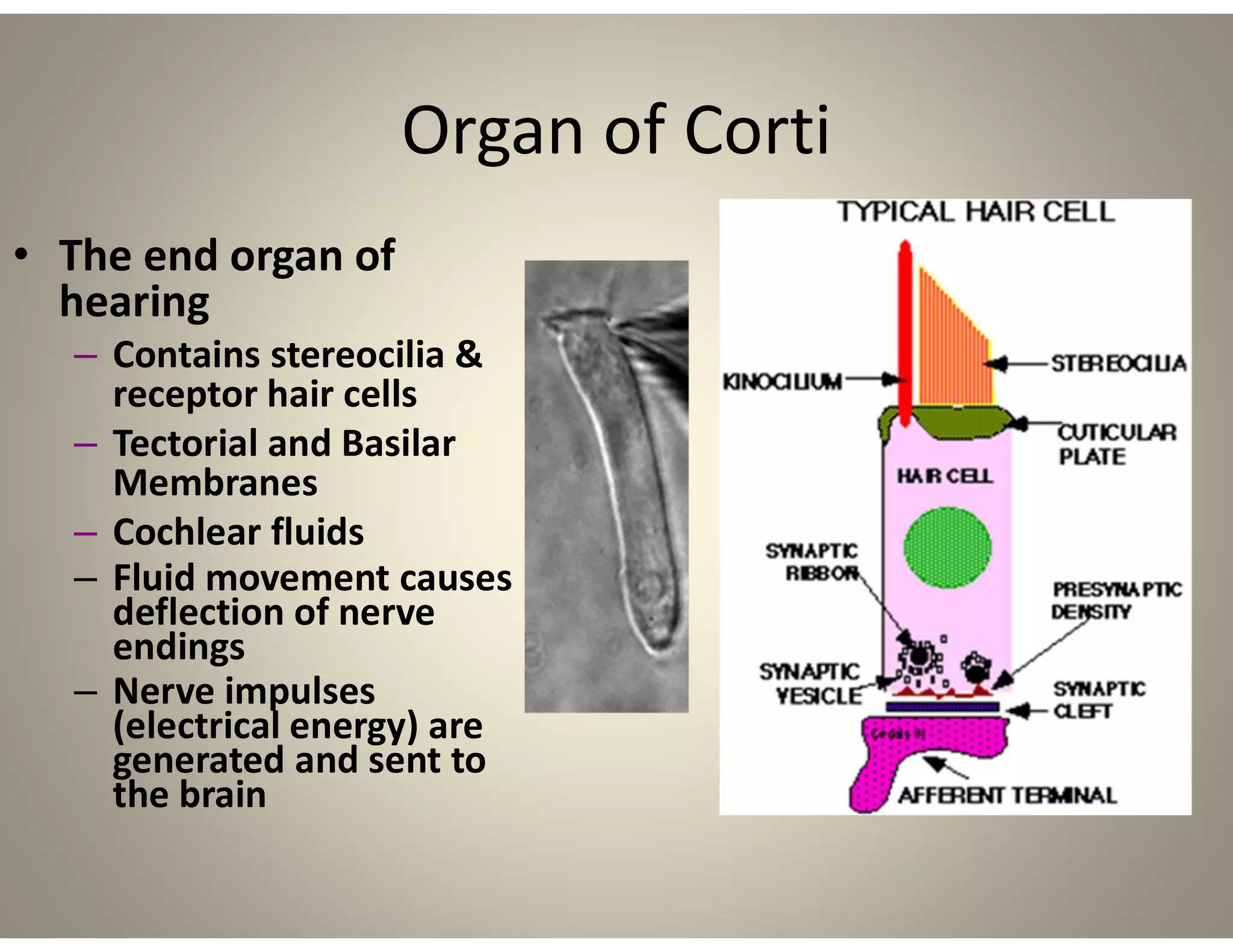
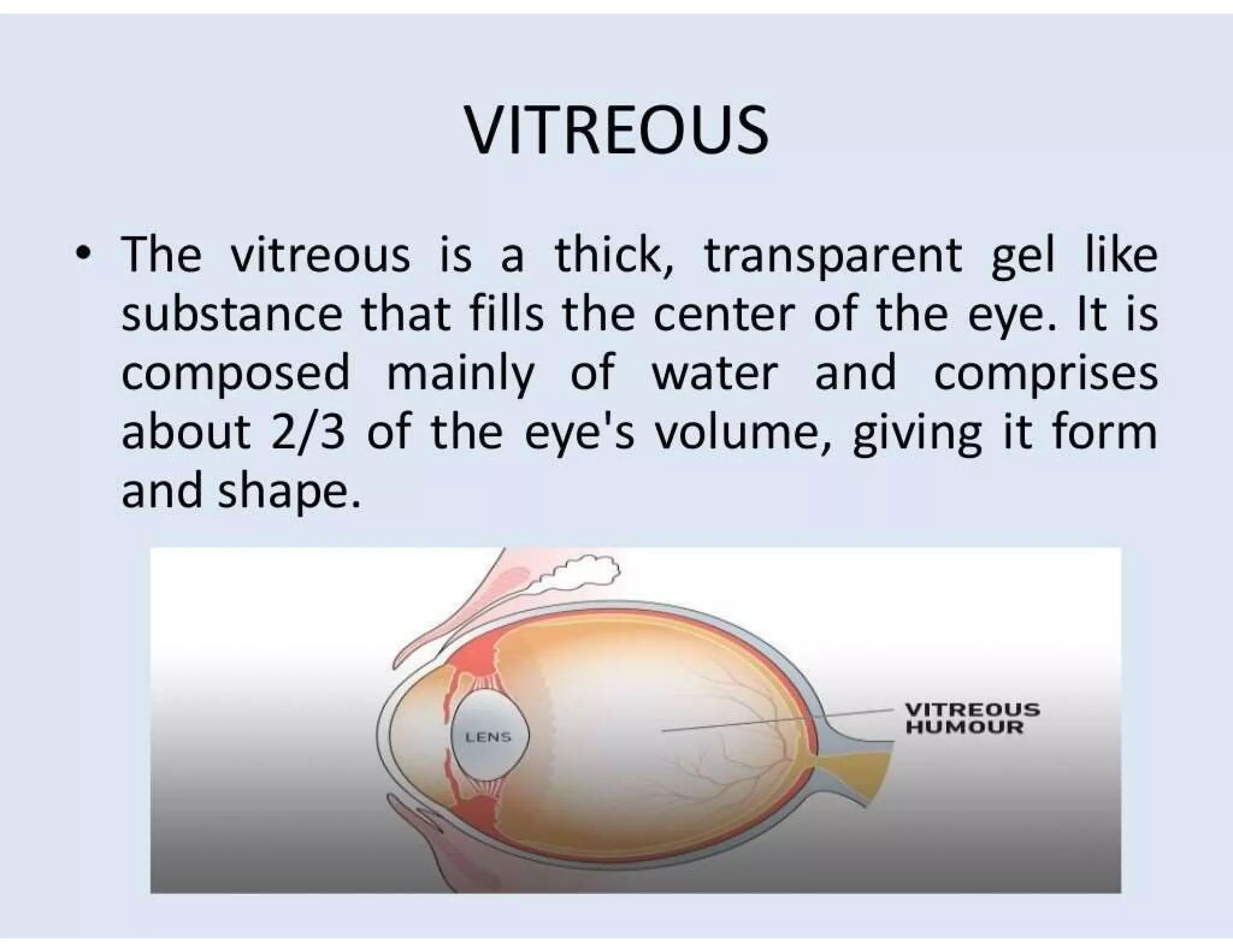
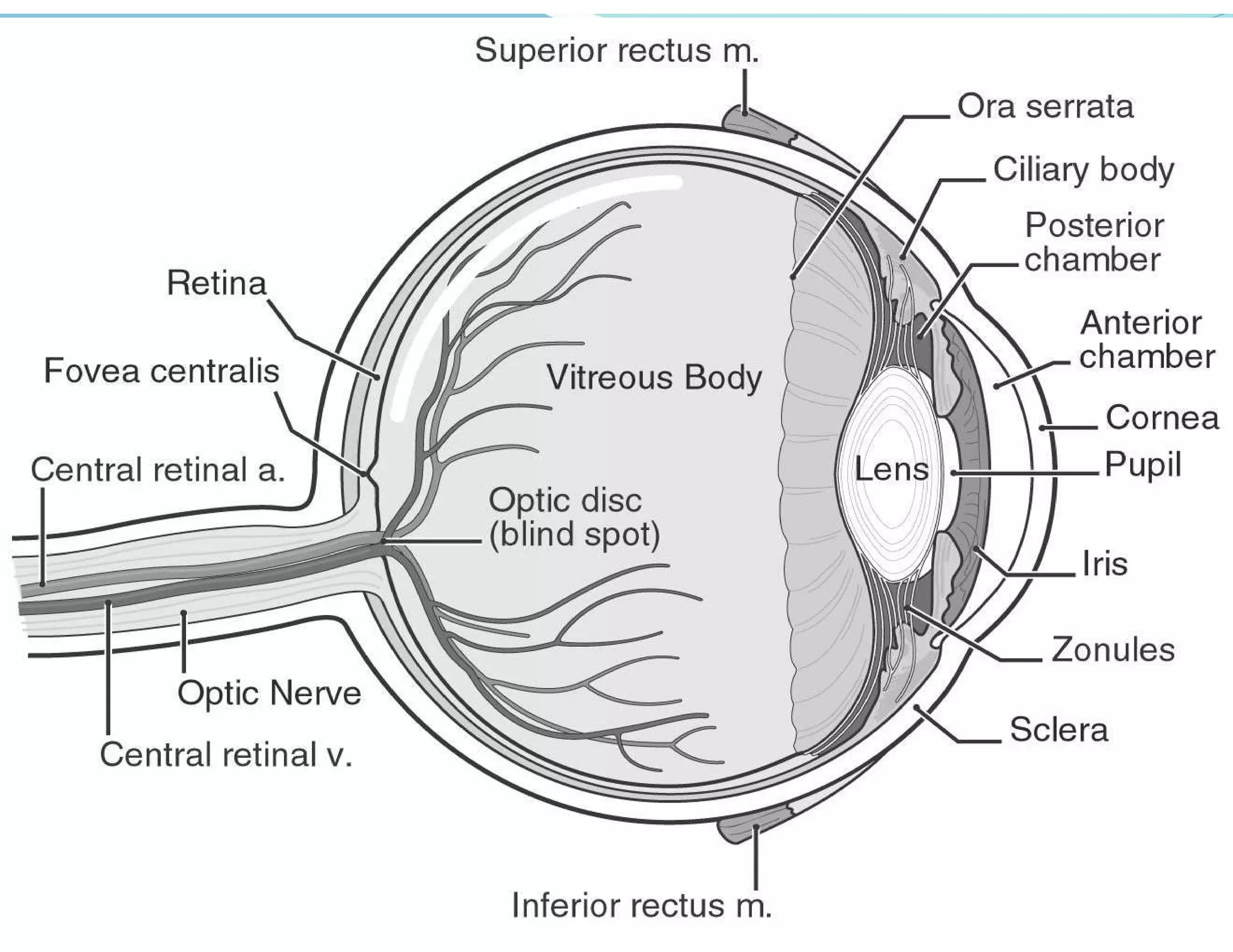
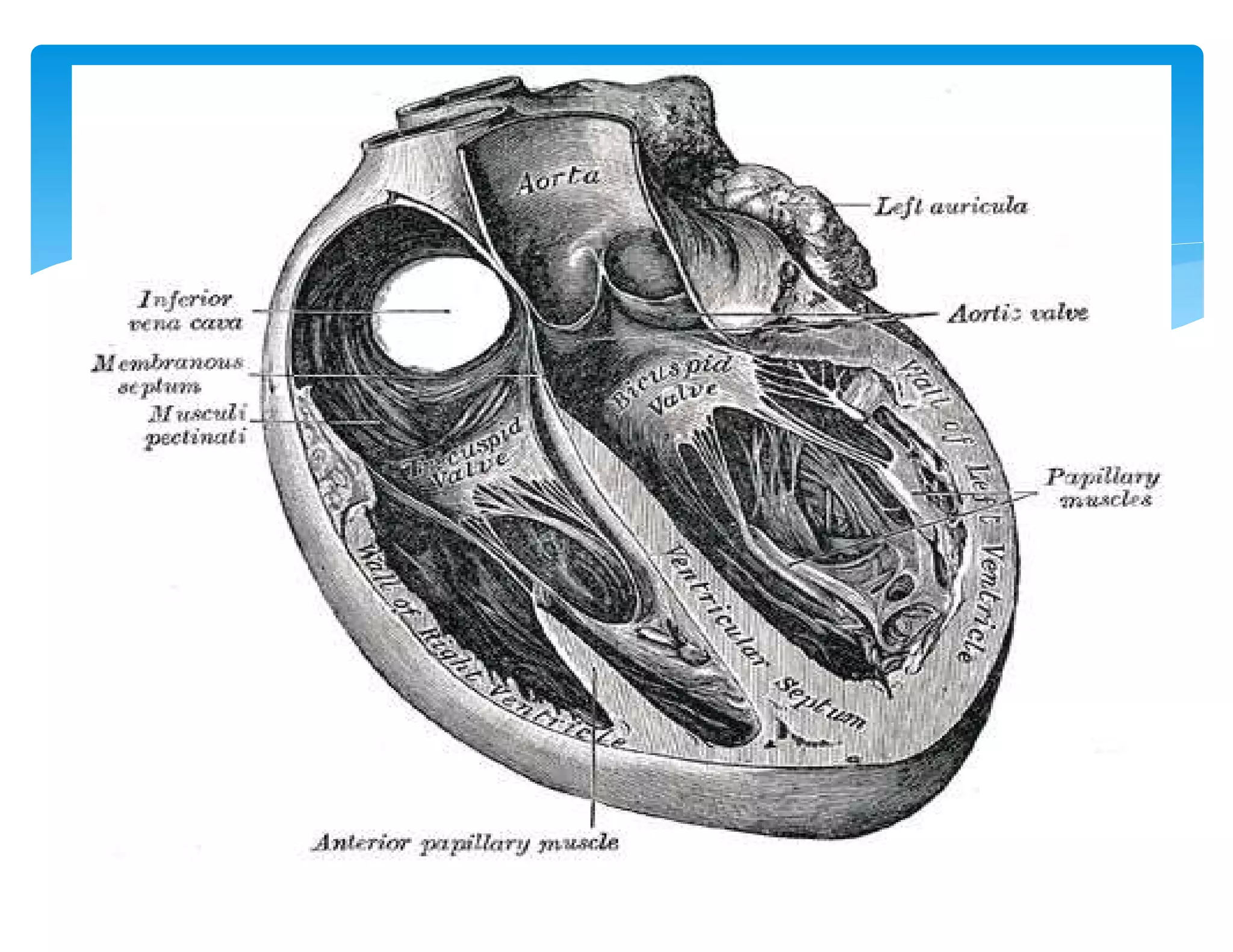
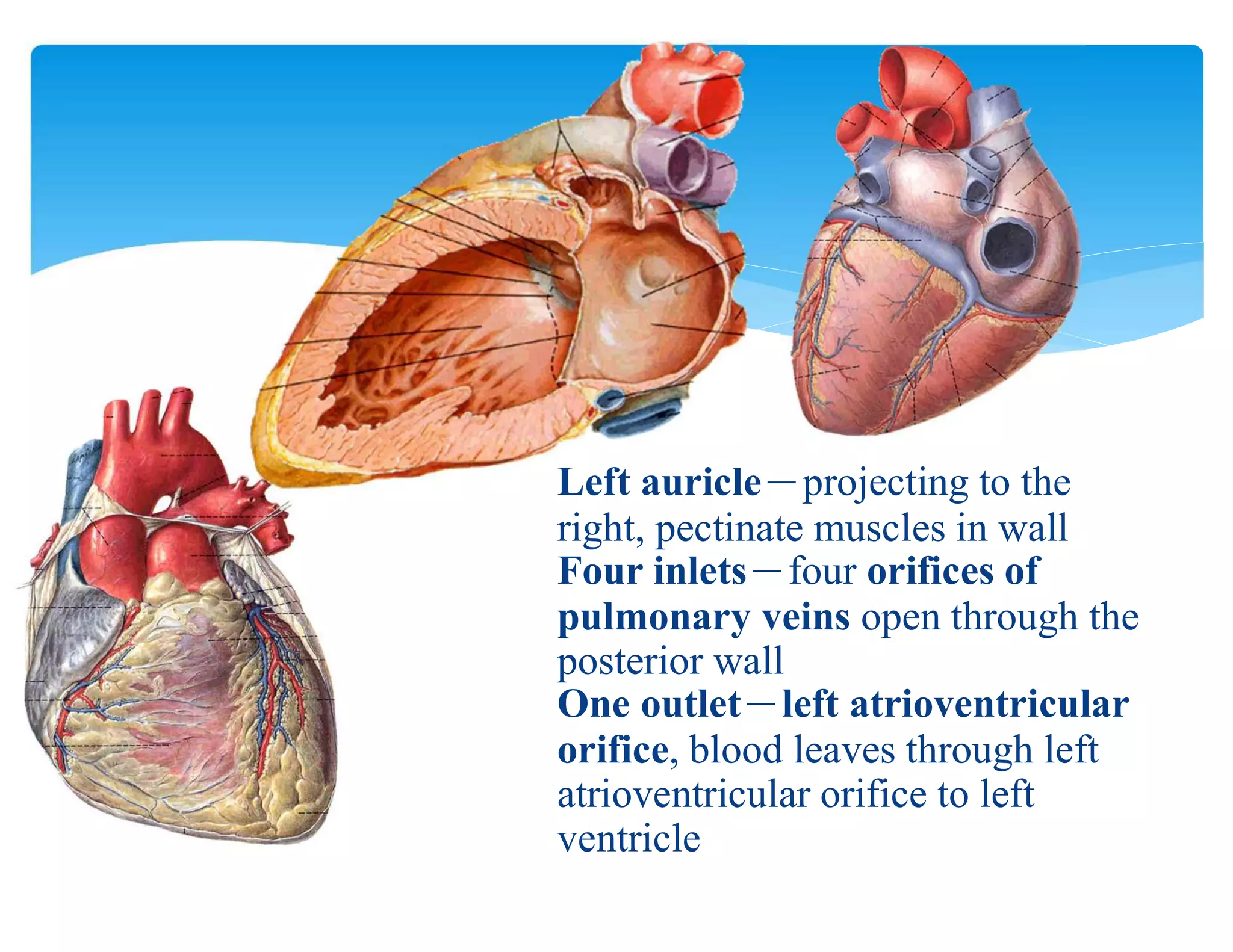
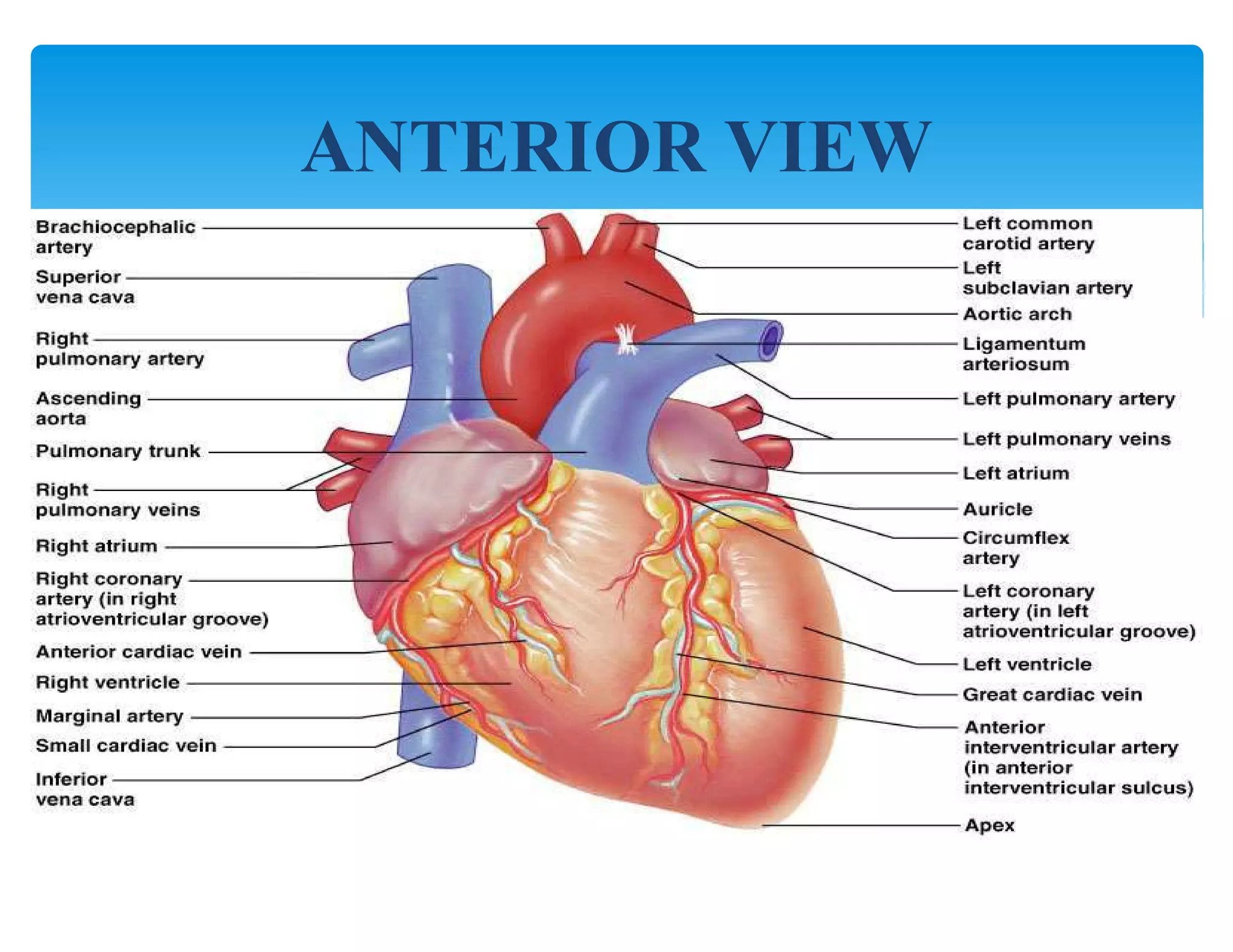
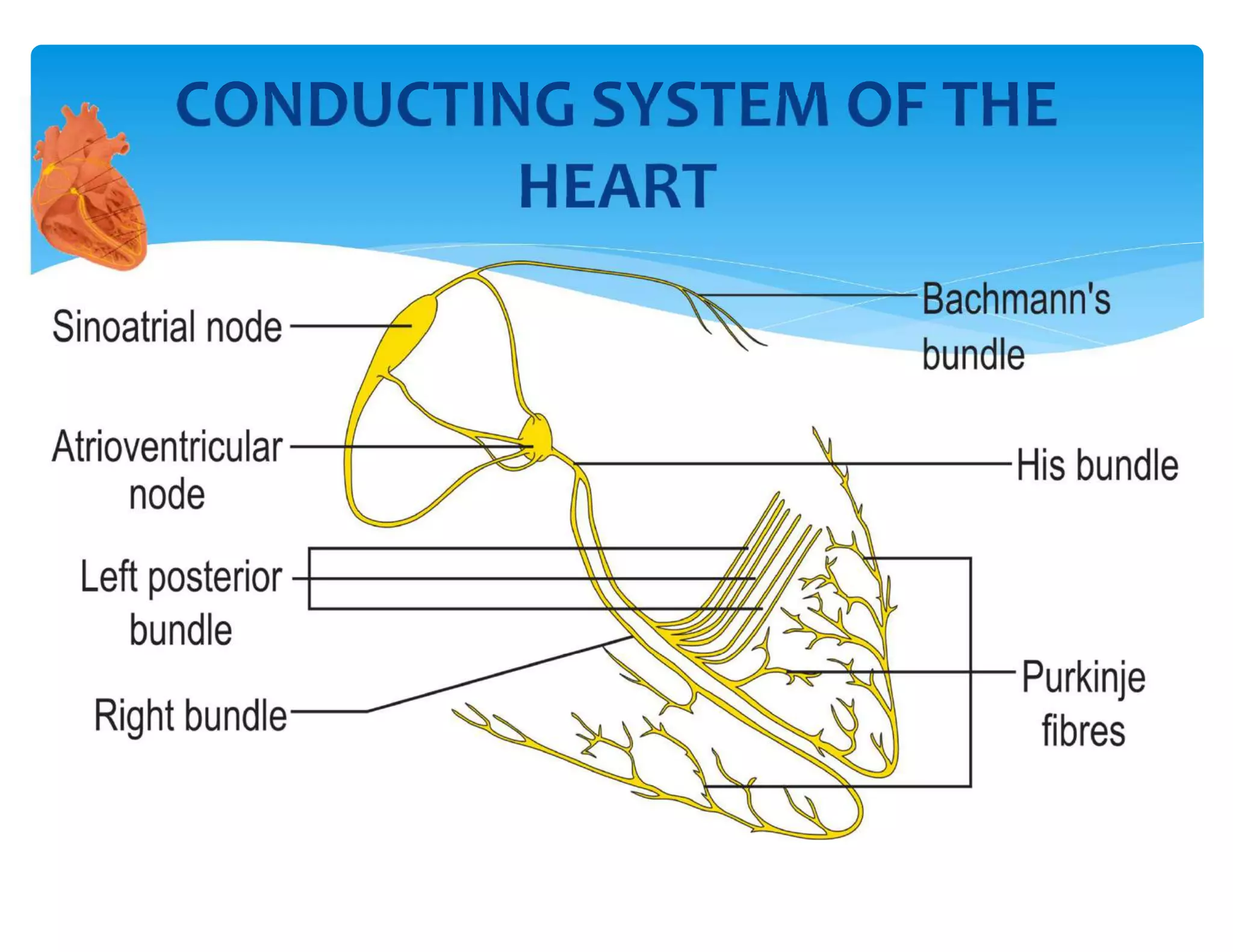
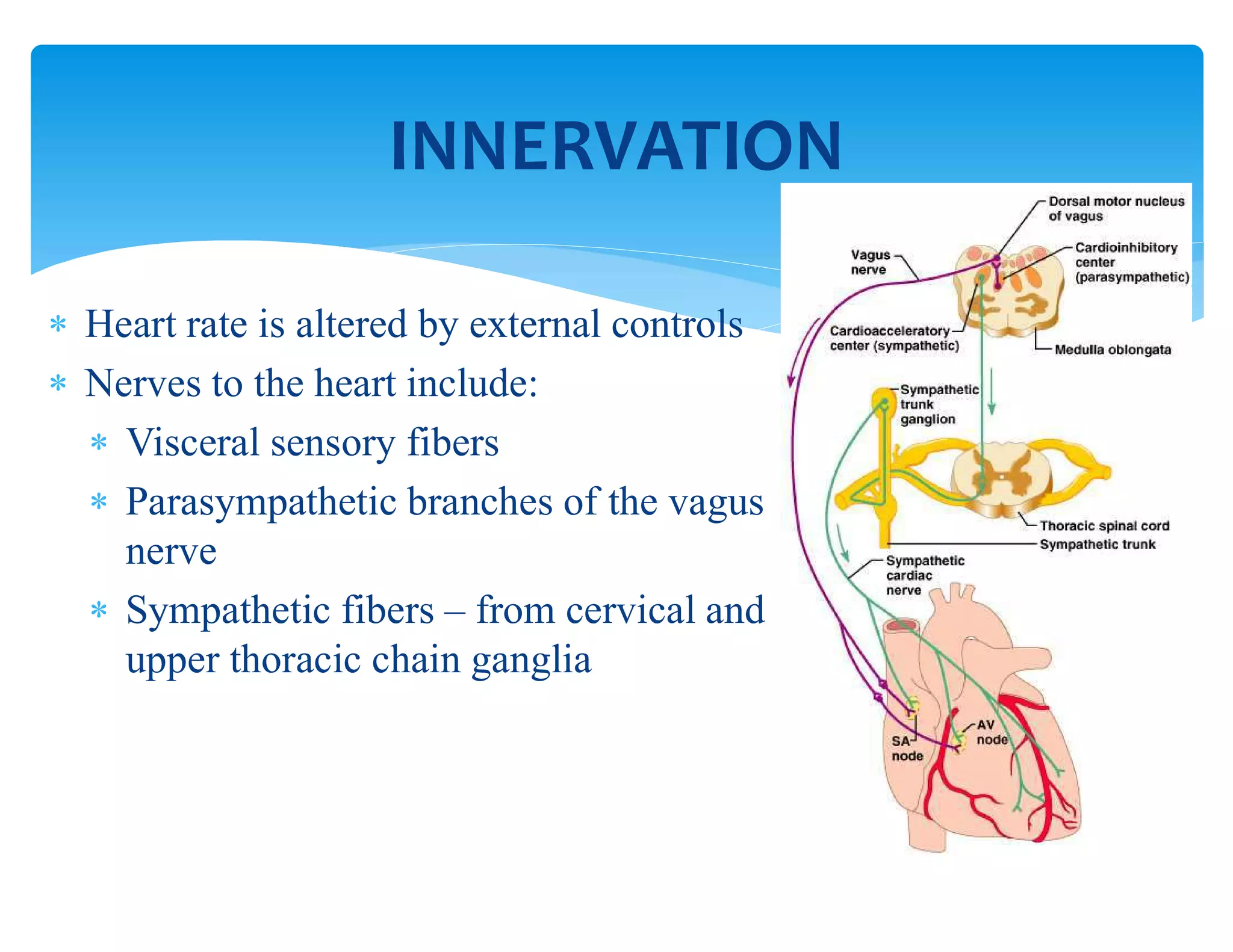
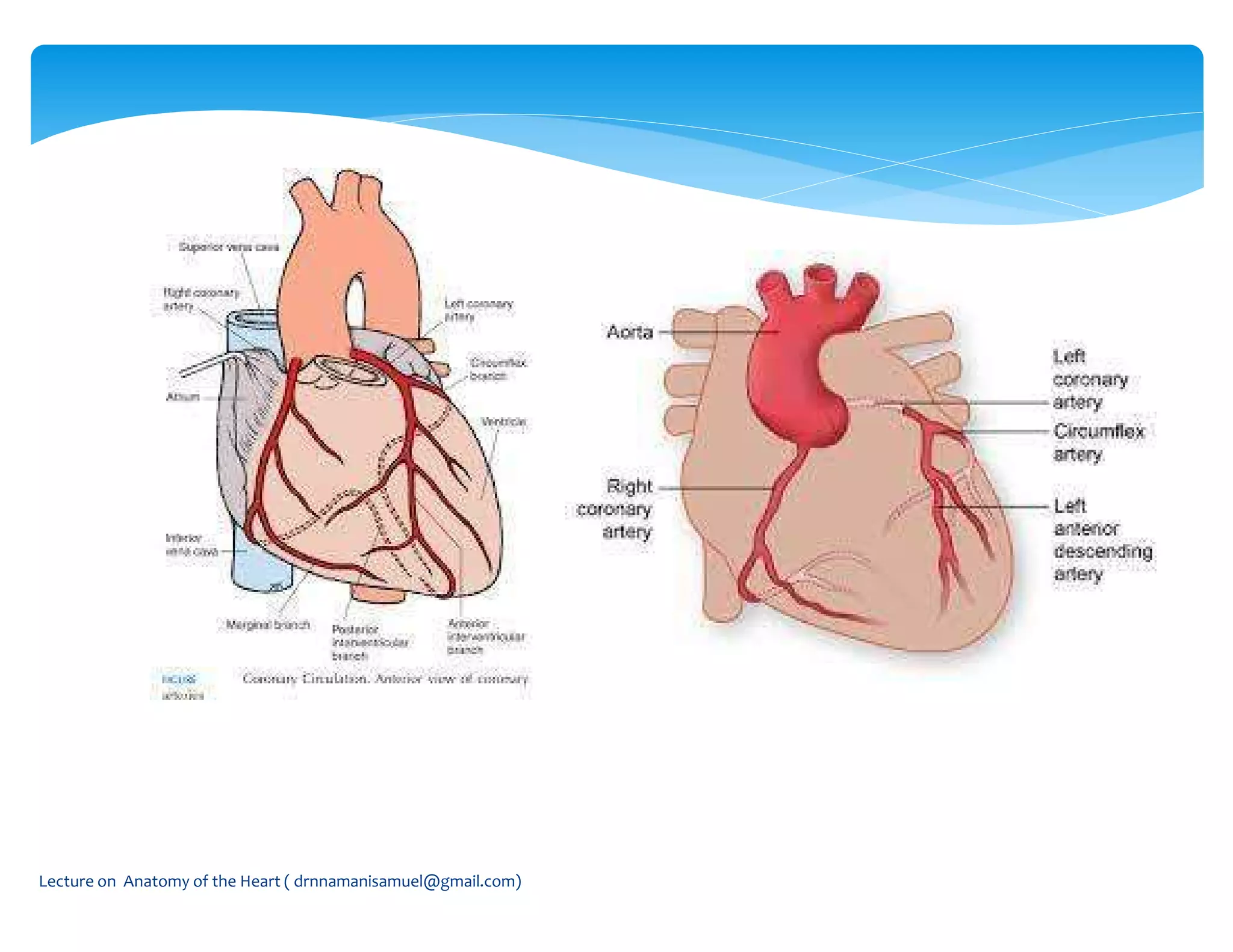
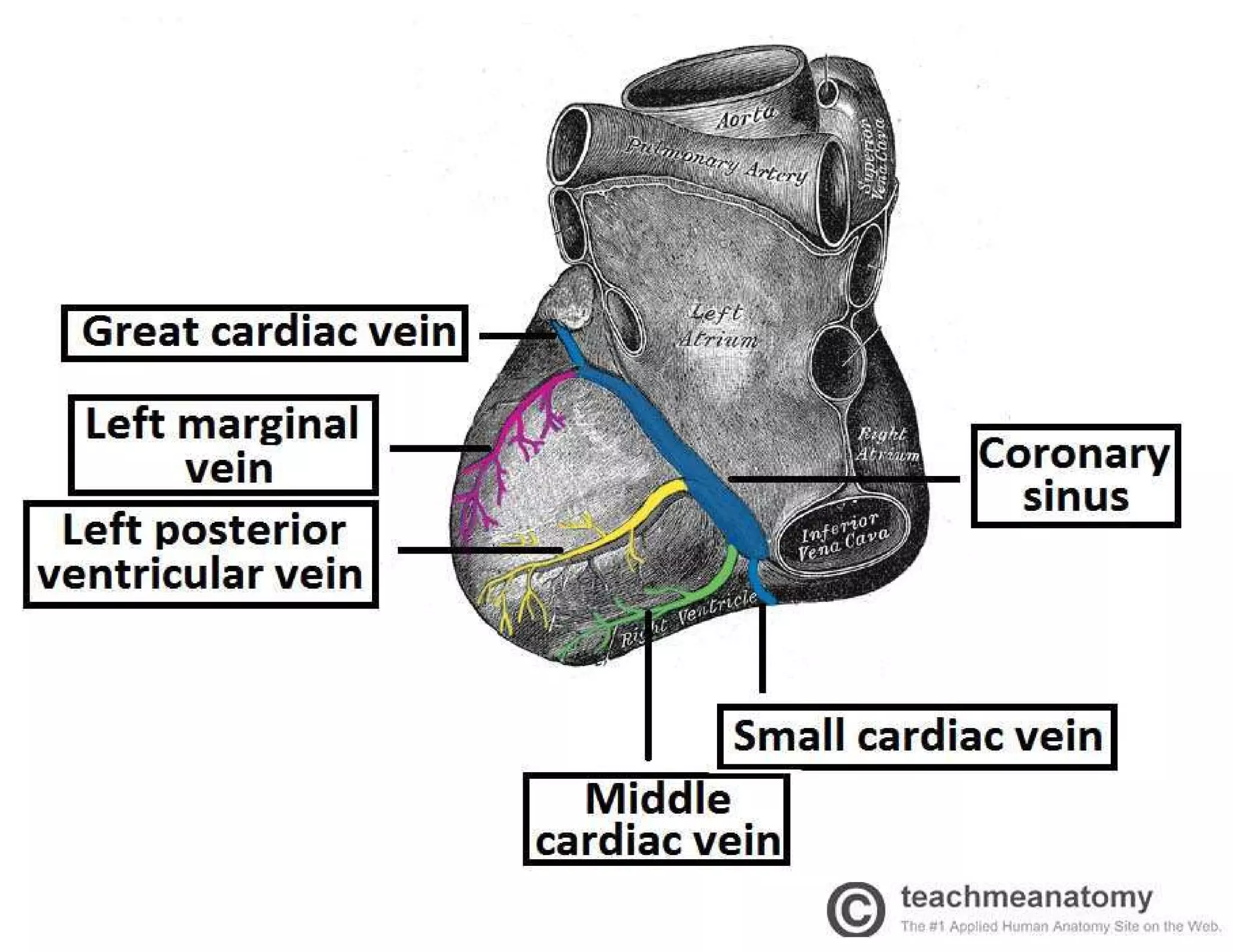
Anatomy of the ear and heart, including structure, blood flow, and sound processing.
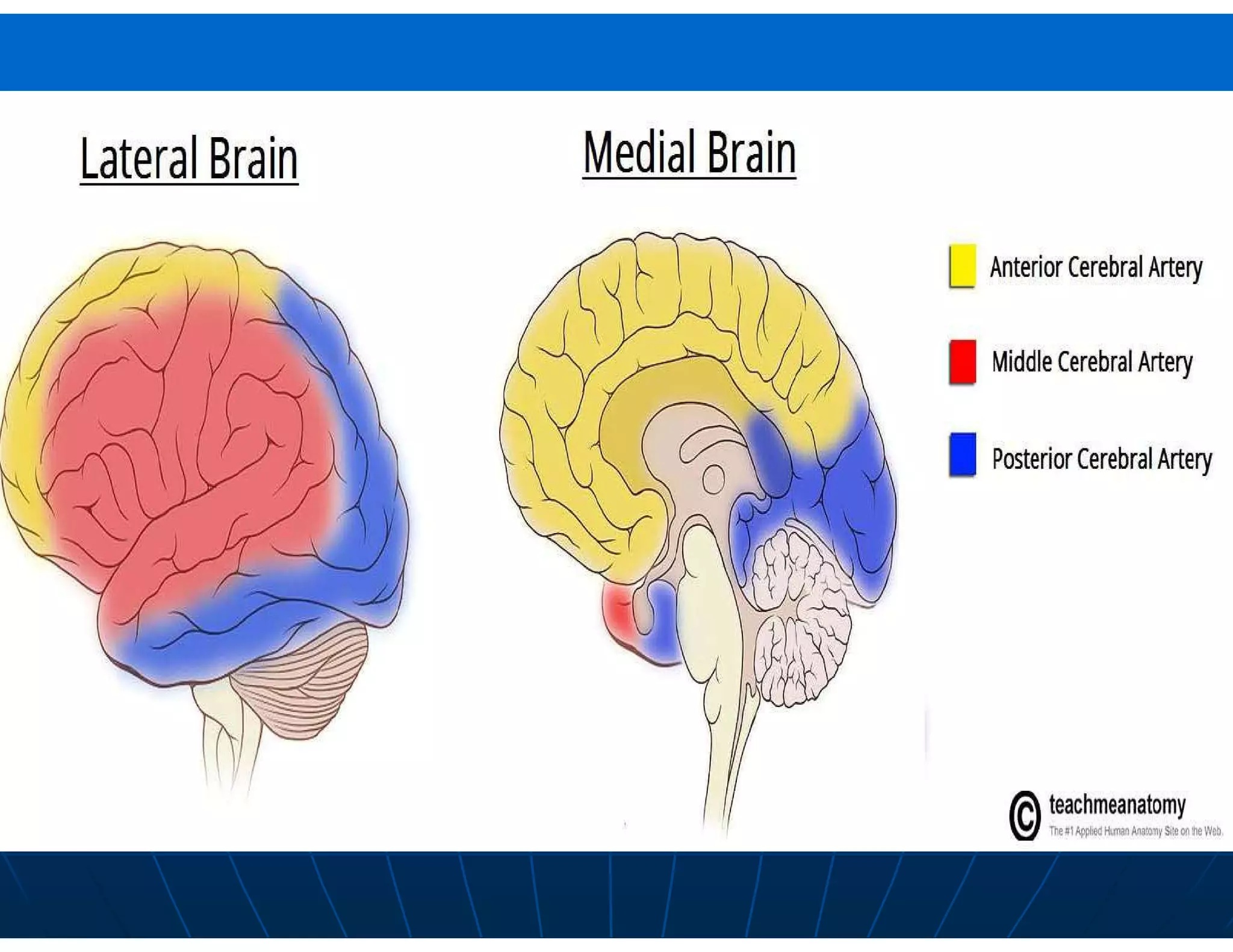
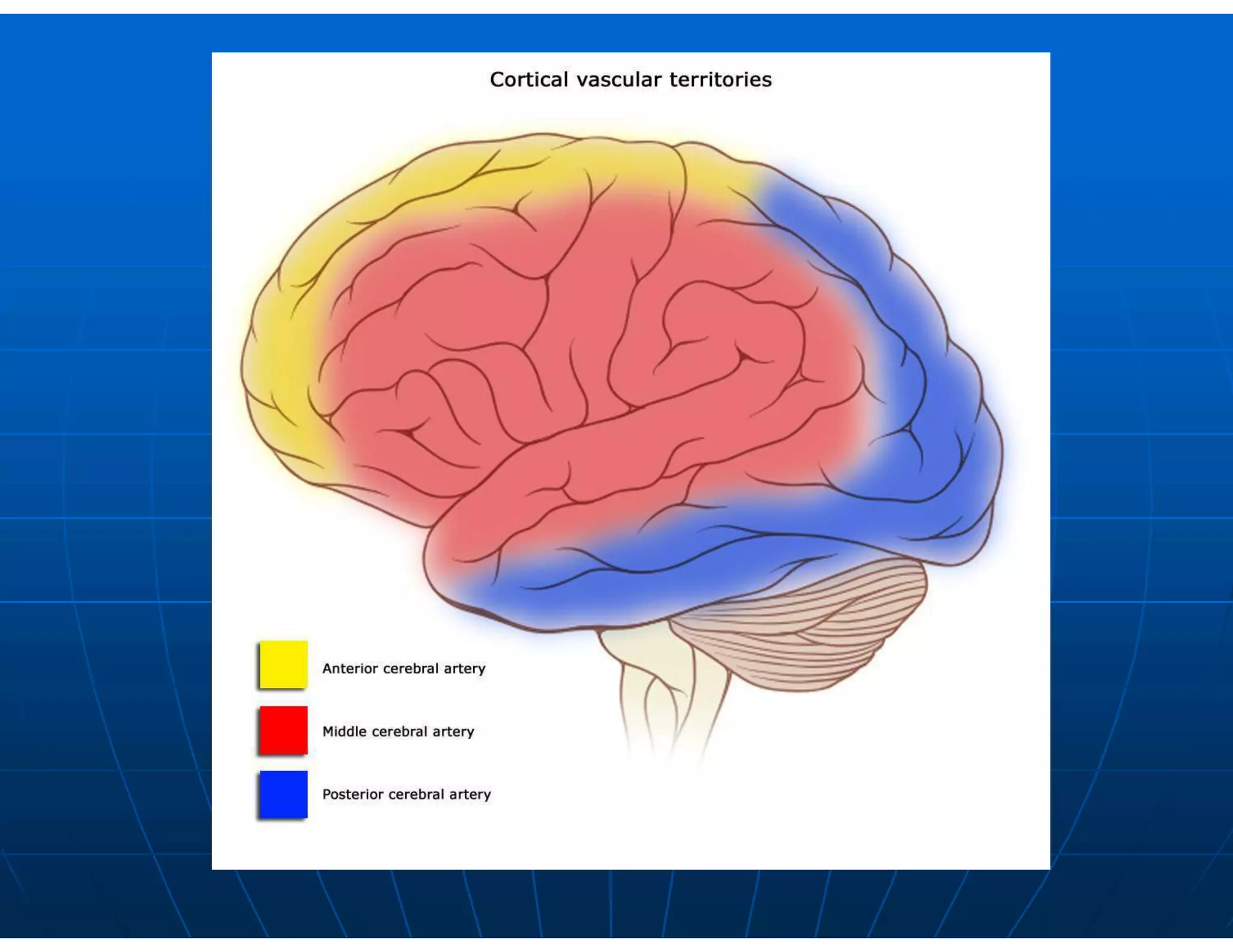
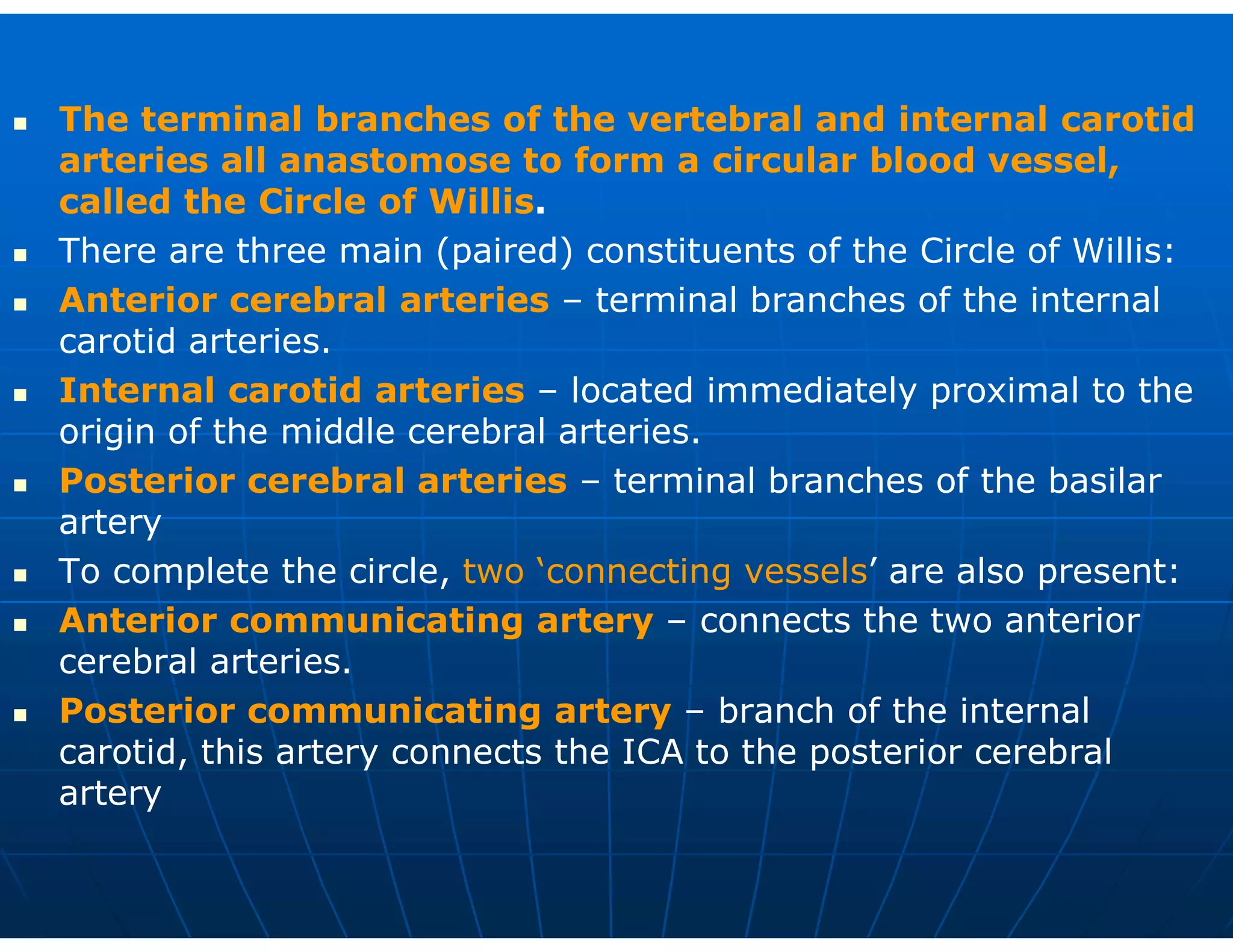
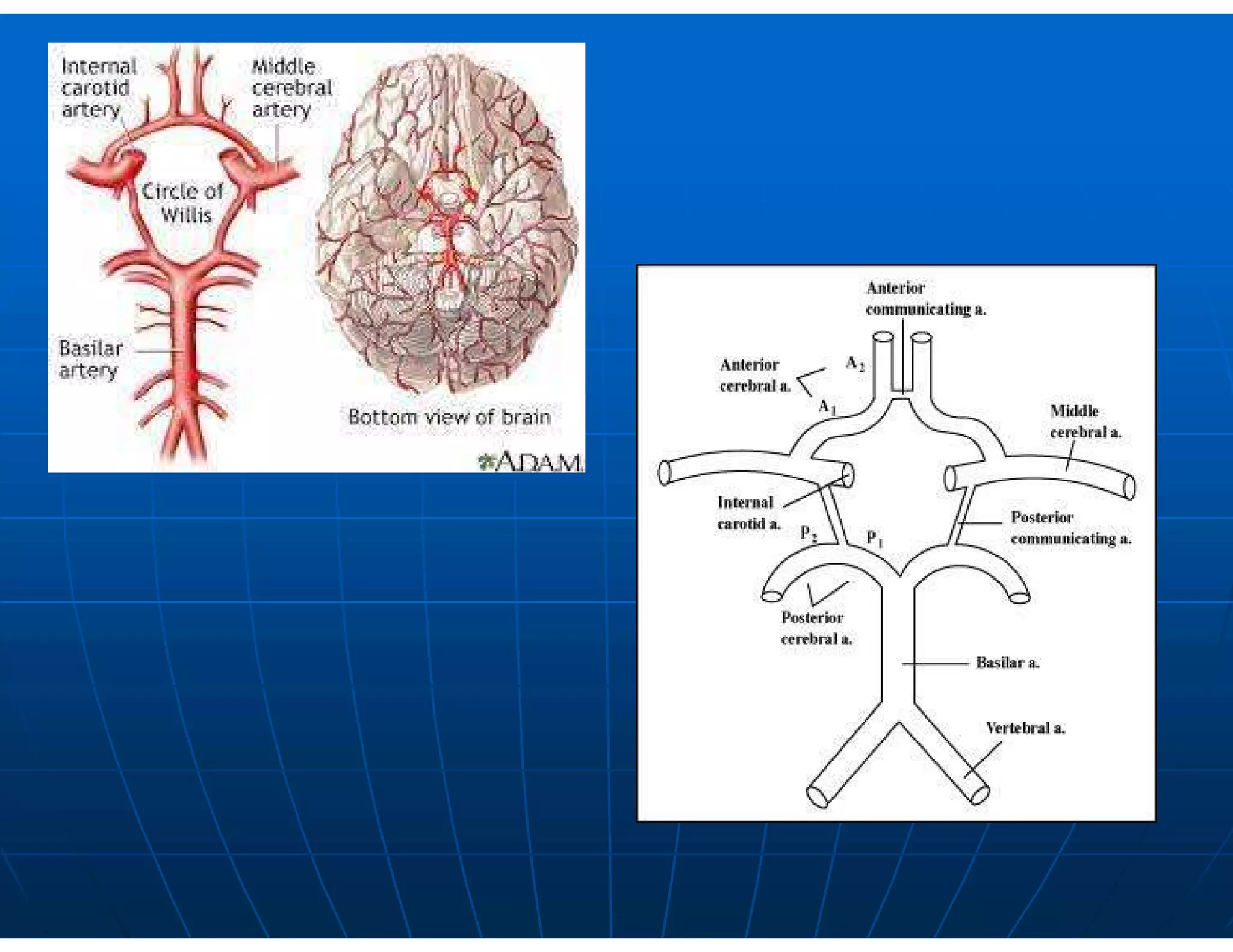
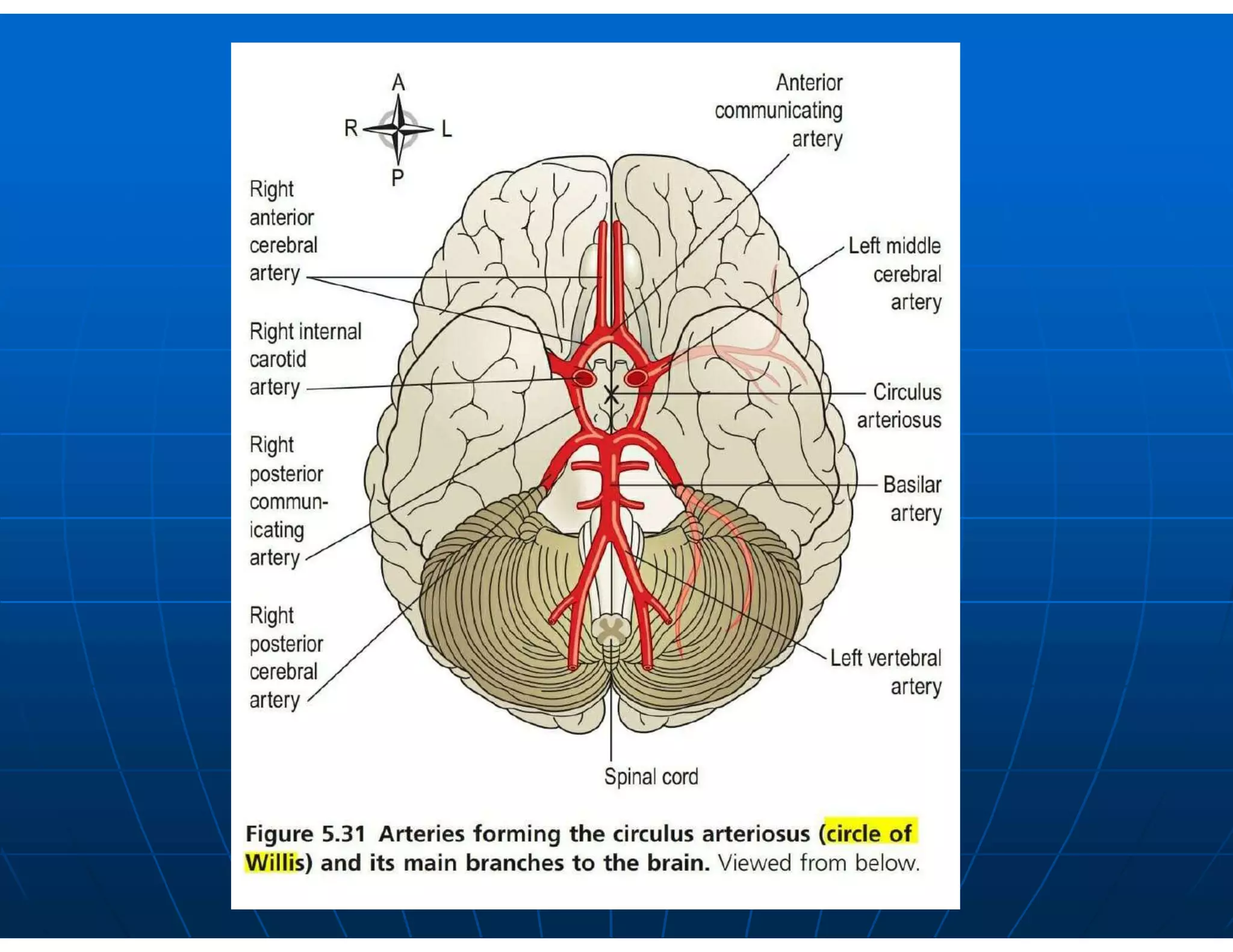
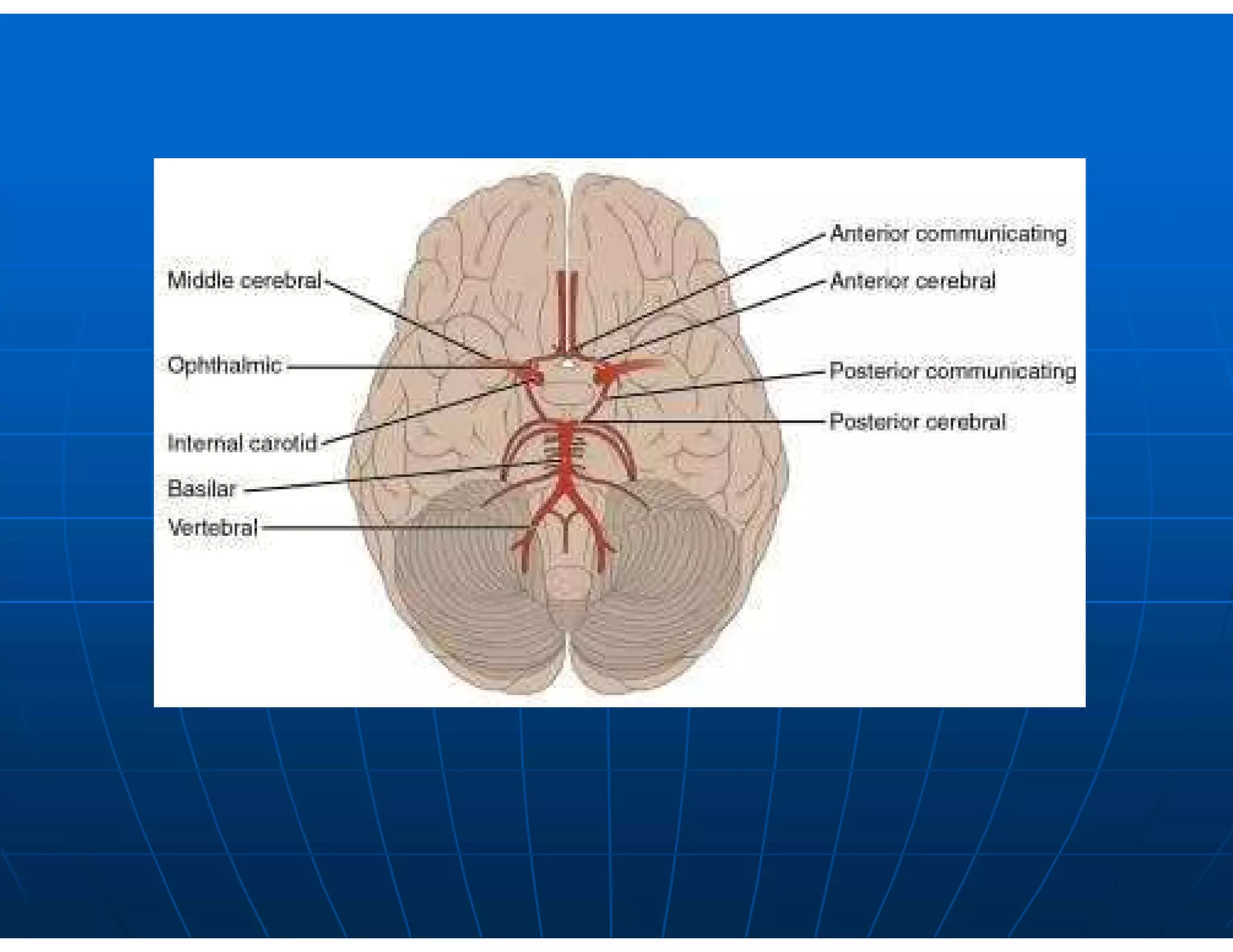
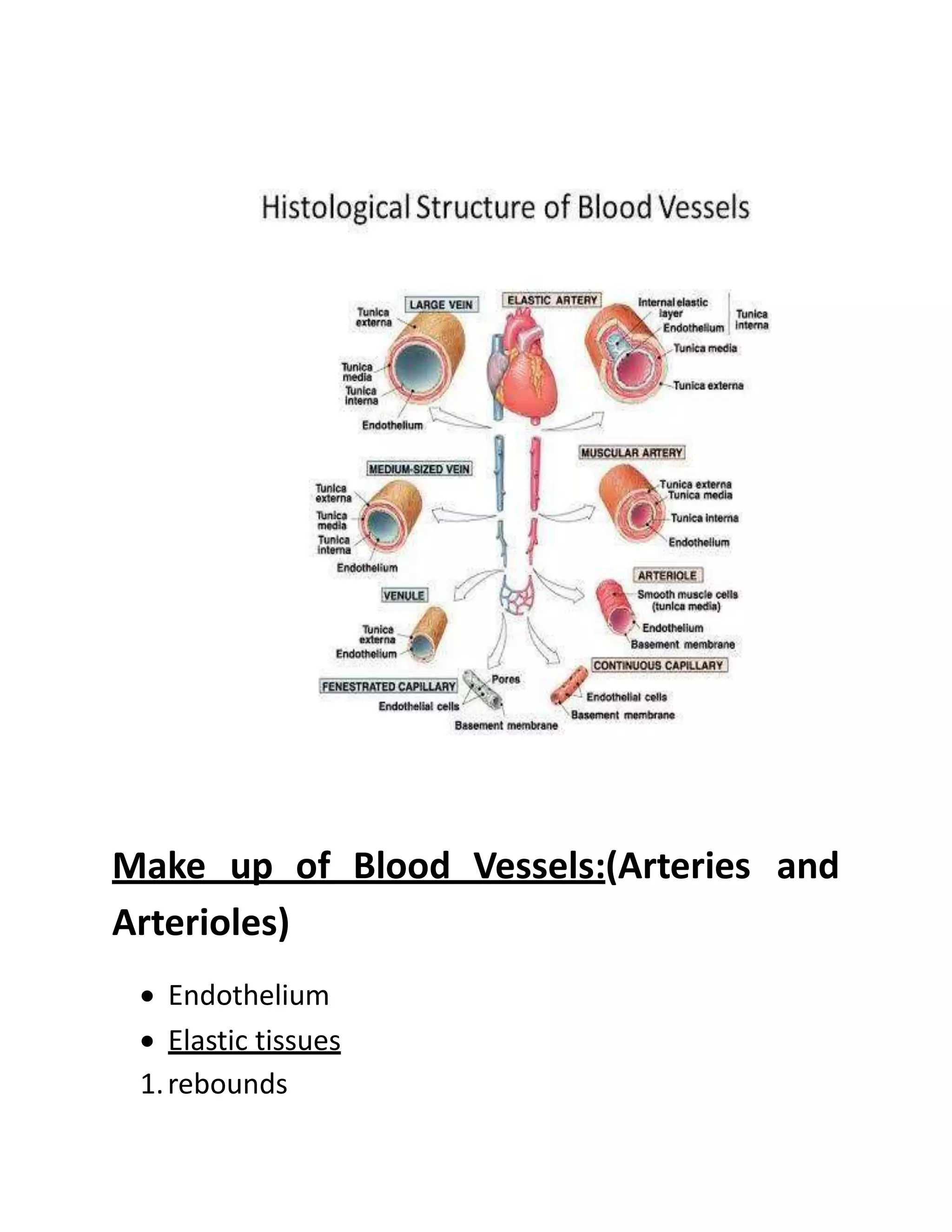
An overview of blood vessels, their structure, types and functions in the circulatory system.