Downloaded 198 times
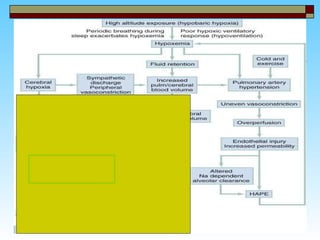
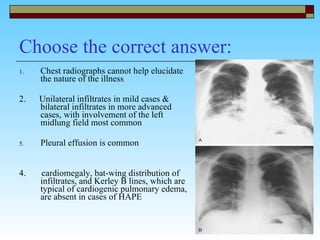


High-altitude medicine deals with illnesses that affect those at high elevations, such as mountaineers and aviators. Acute mountain sickness (AMS) is generally mild and self-limiting, while high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema (HACE) can be life-threatening. Factors like rate of ascent and genetics affect risk. Acclimatization through gradual ascent can help prevent illness by allowing the body to adapt through increased ventilation and other physiological changes. Symptoms, diagnostic criteria, and treatments are described for AMS, HAPE, and HACE.