Downloaded 382 times



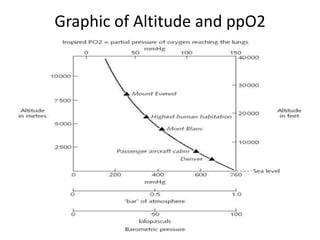






John Muir found being in the mountains calming and spiritual. High altitude was defined as between 1,500-3,500 meters and extreme altitude was above 5,500 meters. The body acclimatizes to high altitude through immediate responses like increased breathing and heart rate, intermediate responses over days like increased red blood cells, and long term responses over weeks like growth of lung capillaries and more efficient use of oxygen. Generations that live at high altitude like Tibetans have developed genetic adaptations through natural selection that augment the acclimatization process.



































































