Downloaded 297 times

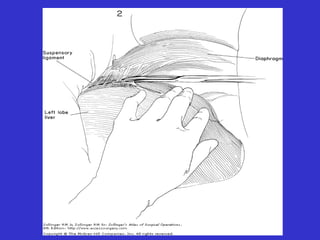
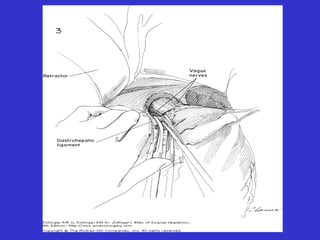
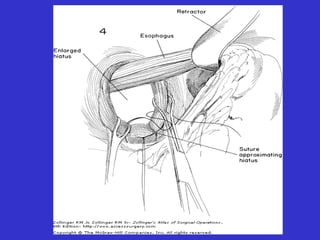
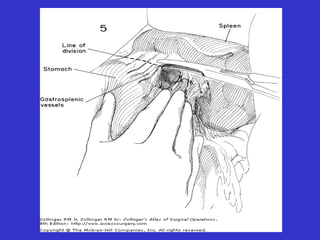
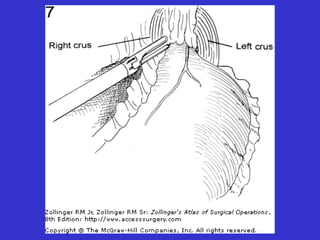
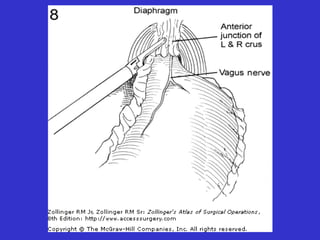
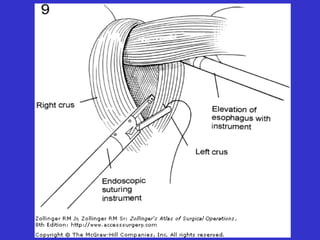
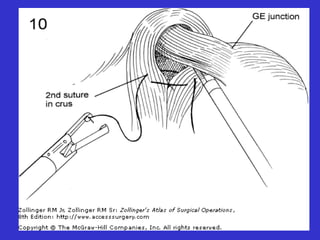


This document provides information about hiatal hernias, including their types and causes. It discusses the clinical presentation of hiatal hernias and methods for diagnosis. Treatment options are medical management or surgical repair, with the surgical approach depending on the hernia type but generally aiming to reduce hernia contents and repair the diaphragmatic defect. Laparoscopic surgery is gaining popularity but may have a higher recurrence rate than open surgery. Outcomes are generally good, with relief of symptoms in most patients after surgical repair.














































































