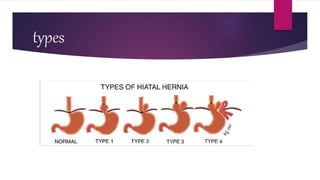
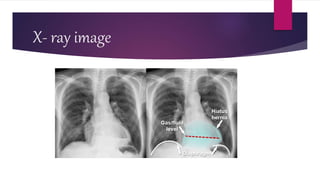
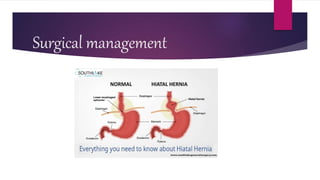
A hiatal hernia occurs when part of the stomach moves through an enlarged opening in the diaphragm. There are two main types: sliding hernias, which are more common, and paraesophageal hernias. Patients may experience heartburn, regurgitation, or dysphagia. Diagnosis involves barium swallow, endoscopy, or CT scan. Treatment focuses on lifestyle changes and medication for symptoms; surgery is recommended for severe cases or complications.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













