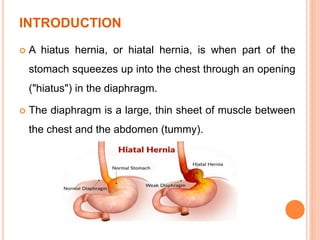
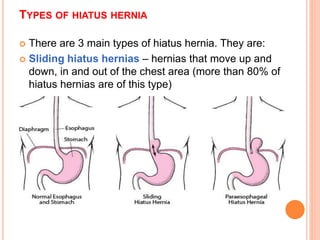
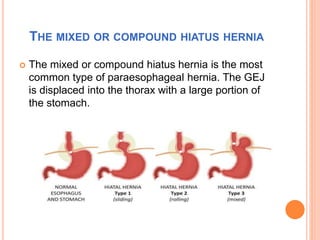
This document discusses hiatal hernia, including its definition, types, causes, symptoms, diagnostic tests, treatment options, nursing care, and potential complications. A hiatal hernia occurs when part of the stomach bulges through an opening in the diaphragm. It can be caused by factors like obesity, smoking, straining, or pregnancy. Symptoms include heartburn, regurgitation, and chest pain. Treatment involves medications to reduce acid production, surgery to repair the hiatal hernia, and lifestyle changes. Nursing care focuses on pain management, education, and preventing acid reflux.