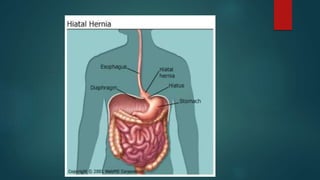
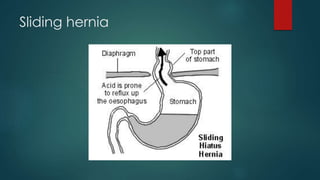
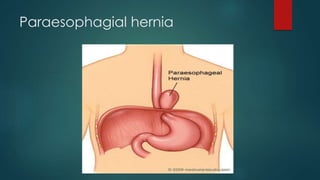
There are two main types of hiatal hernia: sliding and paraesophageal. A sliding hernia occurs when the stomach and lower esophagus slide up into the chest cavity through the diaphragm. A paraesophageal hernia involves part of the stomach squeezing through the diaphragmatic opening and landing next to the esophagus. Hiatal hernias often do not cause symptoms but can sometimes lead to heartburn. Treatment involves lifestyle changes and medication to reduce acid production if heartburn is present. Surgery to repair the diaphragmatic opening may be needed in some cases.