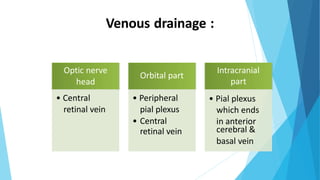
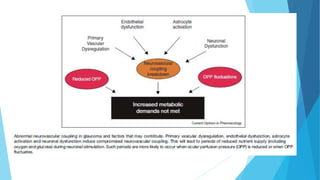
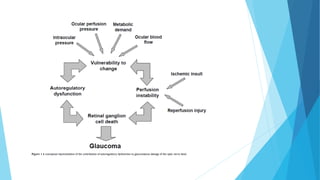
This document discusses ocular blood flow in glaucoma. It provides details on the arterial blood supply and venous drainage of the eye. It describes how glaucoma may be related to low ocular perfusion pressure and abnormalities in ocular blood flow autoregulation. Several studies linking low ocular perfusion pressure to glaucoma risk are summarized. Possible mechanisms like atherosclerosis, vasospasm and endothelial dysfunction that could contribute to impaired ocular blood flow in glaucoma are also outlined.
![Conclusion
Glaucoma is a heterogenous disease comprising multiple etiologies. Alterations in
ocular blood flow have become interestingly implicated in open angle glaucoma
disease pathology.
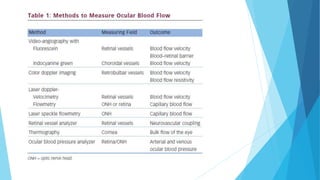
One of the reasons why our understanding of the relation between OPP and glaucoma
is still limited, lies in the difficulties to measure retinal and ONH BF [5, 6].
Doppler optical coherence tomography may become a technique capable of measuring
BF in a valid and reproducible way.
Continuing research is needed to discern the significance of the vascular factors
responsible for glaucoma.
5) Sugiyama T, Araie M, Riva CE, Schmetterer L, Orgul S: Use of laser speckle flowgraphy in ocular blood flow research. Acta
Ophthalmol 2010, 88:723-729.
6)Riva CE, Geiser M, Petrig BL: Ocular blood flow assessment using continuous laser Doppler flowmetry. Acta Ophthalmol
2010, 88:622-629.](https://image.slidesharecdn.com/ocularbloodflowinglaucoma-200624111129/85/Ocular-blood-flow-in-glaucoma-34-320.jpg)
































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














