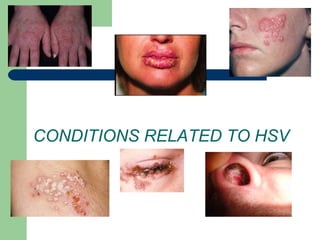
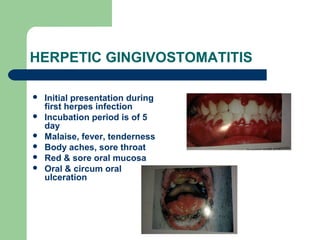
Herpes simplex is caused by one of eight human herpes viruses. It is characterized by initial infection followed by periods of latency and recurrence. There are two types, HSV-1 typically causes oral herpes while HSV-2 typically causes genital herpes. Symptoms vary depending on location of infection but may include lesions, pain, fever and fatigue. Diagnosis is usually based on appearance of lesions but can be confirmed via laboratory tests. While there is no cure, antiviral treatment can reduce symptoms during outbreaks and transmission risk between outbreaks.