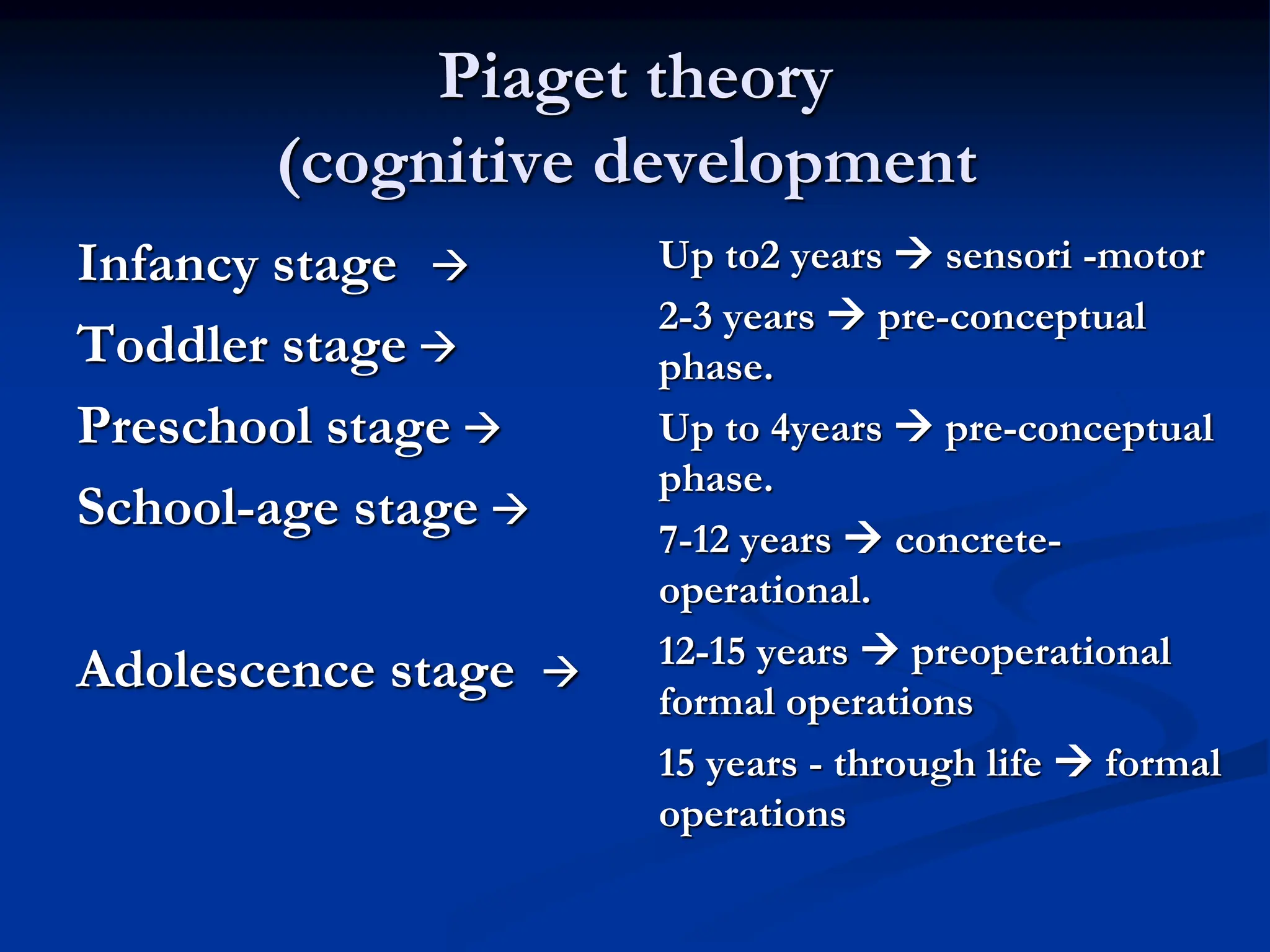
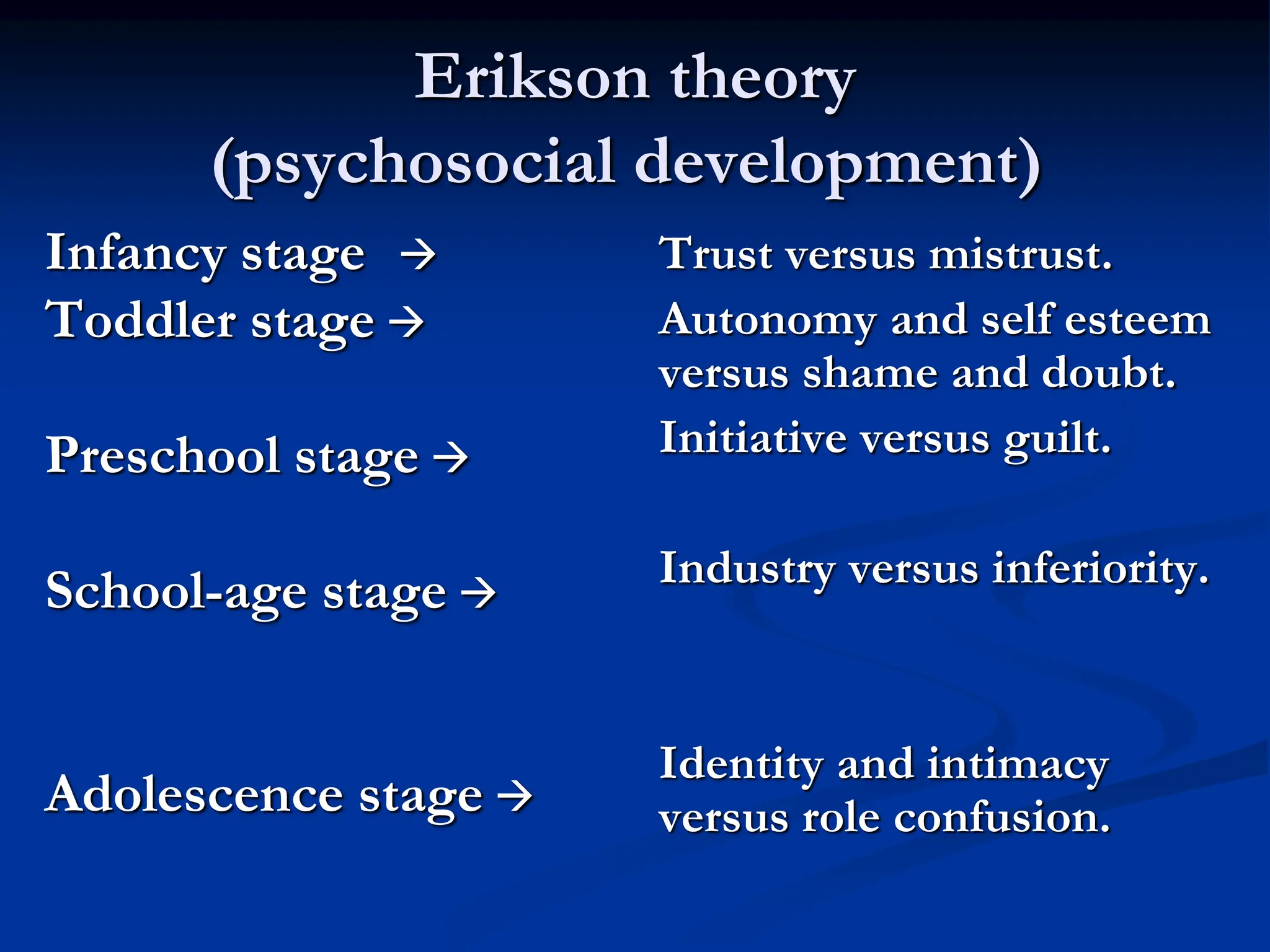
This document discusses growth and development across different childhood stages. It begins with an overview of key concepts like growth, development, and maturation. It then examines the newborn stage in depth, covering physical characteristics, motor and sensory development, and important milestones in the first month. Subsequent sections explore development in infancy, early childhood, middle childhood, and adolescence. For each stage, the document outlines typical physical, cognitive, emotional, social, and motor development.