Downloaded 743 times

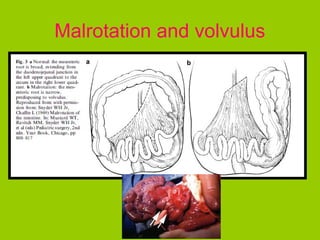




1) Malrotation of the bowel is a common cause of volvulus and obstruction in infants and children, making an accurate diagnosis vital to avoid catastrophic consequences. 2) The normal position of the duodenojejunal junction is to the left of the vertebral body at the level of the duodenal bulb on frontal views and posteriorly on lateral views. 3) A scoring system can help determine if imaging findings are consistent with normal variation, indeterminate for malrotation, or indicative of malrotation based on the number of positive findings present.























































































