Introduction
• The humangastrointestinal (GI) tract is a complex system of serially
connected organs approximately 8 m in length, extending from the
mouth to the anus, which together with its connected secretory
glands, controls the passage, processing, absorption and elimination
of food
4.
Common symptoms ofgastrointestinal and
abdominal disease
• Dysphagia and odynophagia
• Heartburn and reflux
• Indigestion
• Flatulence
• Vomiting
• Anorexia
• Constipation
• Diarrhea
• Abdominal pain
• Abdominal distension
• Weight loss
• Hematemesis
• Rectal bleeding
• Melena
• Jaundice
• Itching
• Urinary symptoms
5.
A. Dysphagia (andodynophagia)
Dysphagia is the awareness of something sticking in the throat or
retrosternally during swallowing; odynophagia is the term that
describes painful swallowing in the oropharynx or esophagus and may
occur with or without dysphagia
B. Heartburn
Heartburn is due to acid reflux from the stomach into the esophagus
It causes pain in the epigastrium, retrosternally and in the neck
6.
Cont..
C. Reflux
Reflux isa symptom which occurs without heartburn, when non-
acidic fluid or bile regurgitates into the mouth, causing a bitter taste
and a disagreeable sensation retrosternally
D. Indigestion (dyspepsia)
Dyspepsia is the medical term for indigestion, a symptom which may
include epigastric pain, heartburn, distension, nausea or ‘an acid
feeling’ occurring after eating or drinking
7.
E. Flatulence
Flatulence describesexcessive wind. It is associated with belching,
abdominal distension and the passage of flatus per rectum
F. Anorexia
Anorexia refers to loss of appetite
G. Constipation
In clinical practice, the passage of formed stool less frequently than
three times per week
8.
Cont..
H. Diarrhea
Is thepassage of loose stools more than three times per day or the
passage of a large amount of stool (more than 300 g/day)
9.
Symptom checklist inpatients with diarrhea
• Is the diarrhea acute, chronic or intermittent?
• Is there tenesmus, urgency or incontinence?
• Is the stool watery, unformed or semisolid?
• Is the stool of large volume and not excessively frequent, suggesting
small bowel disease?
• Is the stool of small volume and excessively frequent, suggesting large
bowel disease?
• Is there blood, mucus or pus associated with the stool?
10.
Cont.
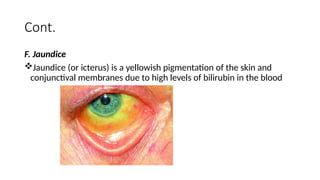
F. Jaundice
Jaundice (oricterus) is a yellowish pigmentation of the skin and
conjunctival membranes due to high levels of bilirubin in the blood
11.
Cont..
J. Hematemesis
Hematemesis isthe vomiting of blood and results from bleeding in
the upper GI tract (above the duodenojejunal flexure)
K. Melena
Melena describes altered blood that has passed through a significant
length of the small bowel and looks jet-black, tarry and has a
characteristic smell
12.
Physical examination ofthe GI tract
and abdomen
• Systemic features of GI disease may be evident on general
examination
13.
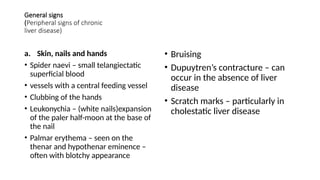
General signs
(Peripheral signsof chronic
liver disease)
a. Skin, nails and hands
• Spider naevi – small telangiectatic
superficial blood
• vessels with a central feeding vessel
• Clubbing of the hands
• Leukonychia – (white nails)expansion
of the paler half-moon at the base of
the nail
• Palmar erythema – seen on the
thenar and hypothenar eminence –
often with blotchy appearance
• Bruising
• Dupuytren’s contracture – can
occur in the absence of liver
disease
• Scratch marks – particularly in
cholestatic liver disease
14.
b. Endocrine –due to excess estrogens
• Gynecomastia
• Testicular atrophy
• Loss of axillary and pubic hair
15.
1. Inspection
• Thepatient should be lying supine with arms loosely at the sides, the
head and neck supported by pillows, sufficient for comfort
• Make sure there is a good light, that the room is warm and that the
hands are warm
• Stand on the patient’s right side, introduce yourself to the patient and
with his consent expose the abdomen by turning down all the bed
clothes except the upper sheet
• The clothing should then be drawn up to just above the xiphisternum
and the sheet folded down to the level of the symphysis pubis
16.
Cont..
• inspection ofthe groins and genitalia must not be neglected and
needs to be carried out with discretion, with full explanation as to the
reasons, and leaving these areas exposed for the minimum time
17.
Things to noteon inspection
1. Shape of the abdomen
2. Shape of the umbilicus
3. Movements of the abdominal wall
4. Skin and surface of the abdomen
18.
1. Shape ofthe abdomen
• Is the abdomen of normal contour and fullness, or distended? Is it
scaphoid (sunken)?
• Generalized fullness or distension may be due to fat, fluid, flatus,
faeces or fetus
• Localized distension may be symmetrical and centered around the
umbilicus as in the case of small bowel obstruction, or asymmetrical
as in gross enlargement of the spleen, liver or ovary
19.
2. Shape ofthe umbilicus
• Normally the umbilicus is slightly retracted and inverted
• If it is everted, then a umbilical hernia may be present and this can be
confirmed by feeling an expansile impulse on palpation of the swelling
when the patient coughs
• The hernia sac may contain omentum, bowel or fluid
20.
3. Movements ofthe abdominal wall
• Normally there is a gentle rise in the abdominal wall during
inspiration and a fall during expiration; the movement should be free
and equal on both sides
• In generalized peritonitis, this movement is absent or markedly
diminished (the ‘still, silent abdomen’)
• To aid the recognition of intra-abdominal movements, shine a light
across the patient’s abdomen. Even small movements of the intestine
may then be detected by alterations in the pattern of shadows cast
over the abdomen
21.
4. Skin andsurface of the abdomen
• In marked abdominal distension, the skin is smooth and shiny
• Striae atrophica or gravidarum are white or pink wrinkled linear marks
on the abdominal skin
• They are produced by gross stretching of the skin with rupture of the
elastic fibres and indicate a recent change in size of the abdomen,
such as is found in pregnancy, ascites, wasting diseases and severe
dieting
• Wide purple striae are characteristic of Cushing’s syndrome and
excessive steroid treatment
22.
Cont..
• Note anyscars present, their site, whether they are old (white) or
recent (red or pink), linear or stretched (and therefore likely to be
weak and contain an incisional hernia)
23.
2. Auscultation
• Auscultationof the abdomen is for detecting bowel sounds and vascular
bruits
• With the patient lying on his back, place the stethoscope diaphragm to the
right and bellow the umbilicus and do not move it
• Bowel sounds are gurgling noises from the normal peristaltic activity of the
gut. They normally occur every 5-10 seconds, but the frequency varies.
Listen for up to 2 minutes before concluding that bowel sounds are absent
• Absence of bowel sounds implies paralytic ileus or peritonitis. In intestinal
obstruction, bowel sounds occur with increased frequency, volume and
pitch, and have a high-pitched, tinkling quality
24.
Cont..
• A succussionsplash may be heard without a stethoscope and also on
auscultation when there is pyloric stenosis, in advanced intestinal
obstruction with grossly distended loops of bowel and in paralytic
ileus
• Have the patient lie supine and place the stethoscope over the
epigastrium. Shake the abdomen briskly from side to side and, if the
stomach is distended with fluid, a splashing sound will be heard
25.
Cont..
Vascular bruits
• Listenfor bruits by light application of the stethoscope above and to
the left of the umbilicus (aorta), the iliac fossae (iliac arteries),
epigastrium (coeliac or superior mesenteric arteries), laterally in the
midabdomen (renal arteries) or over the liver (increased blood flow in
liver tumors – classically primary liver cancer)
• If an arterial bruit is heard, it is a significant finding which indicates
turbulent flow in the underlying vessel, due to stenosis, aneurysm or
a malignant circulation
26.
3. Percussion
• Thenormal percussion note over most of the abdomen is resonant
(tympanic) except over the liver, where the note is dull. A normal
spleen is not large enough to render the percussion note dull.
• A resonant percussion note over suspected enlargement of liver or
spleen weighs against there being true enlargement
1. liver
• Theupper and lower borders of the right lobe of the liver can be
mapped out accurately by percussion
• Start anteriorly, at the fourth intercostal space, where the note will be
resonant over the lungs, and work vertically downwards
• Over a normal liver, percussion will detect the upper border, which is
found at about the fifth intercostal space (just below the right nipple
in men). The dullness extends down to the lower border at or just
below the right subcostal margin, giving a normal liver vertical height
of 12-15 cm
29.
2. Spleen
• Percussionover a substantially enlarged spleen provides rapid
confirmation of the findings detected on Palpation
• Dullness extends from the left lower ribs into the left hypochondria
and left lumbar region
30.
3. Urinary bladder
•The findings in a patient with retention of urine are usually
unmistakable on palpation
• The dullness on percussion and clear difference from the adjacent
bowel provides reassurance that the swelling is cystic or solid and not
gaseous
31.
Detection of ascites
•Findings on percussion of the abdomen
• Shifting dullness:
• lie the patient supine
• Place your fingers on the longitudinal axis on the midline near the umbilicus and
begin percussion moving your fingers laterally towards the right flank
• When dullness is first detected keep your fingers in that position and ask the patient
to roll on their left side
• Wait a few seconds for any peritoneal fluid to redistribute
• Percuss again starting at the place that you stopped
• With ascites, this place should now be resonant rather than dull
• Continue to percuss back towards the midline until you find the area of dullness
again (this confirms that fluid did actually shift)
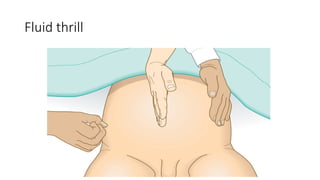
Detection of ascites
•Fluid Thrill
• Lie the patient supine
• Place one hand flat over the lumbar region on one side of the abdomen
• Ask an assistant to put the side of their hand longitudinally and firmly in the
midline of the abdomen (this will dampen any movement that is transmitted
through the fat of the abdominal wall itself)
• Flick or tap the opposite lumbar region
• If the patient has ascites, a fluid thrill or wave is felt by the detecting hand
held flat on the lumbar region
PALPATION
• Tell thepatient to relax as best they can and to breathe quietly, and
assure them that you will be as gentle as possible.
• Enquire about the site of any pain and come to this region last.
• When palpating, the wrist and forearm should be in the same
horizontal plane where possible, even if this means bending down or
kneeling by the patient's side.
• The best palpation technique involves moulding the relaxed right
hand to the abdominal wall, not to hold it rigid
36.
Cont..
• The bestmovement is gentle but with firm pressure, with the fingers
held almost straight but with slight flexion at the
metacarpophalangeal joints, and certainly avoid sudden poking with
the fingertips
Cont..
• It ishelpful to have a logical sequence to follow and, if this is done as
a matter of routine, then no important point will be omitted.
• The following scheme is suggested, which may need to be varied
according to the site of any pain:
Start in the left lower quadrant of the abdomen, palpating lightly, and
repeat for each quadrant.
Repeat using slightly deeper palpation examining each of the nine
areas of the abdomen
39.
cont..
Feel forthe left kidney.
Feel for the spleen.
Feel for the right kidney.
Feel for the liver.
Feel for the urinary bladder.
Feel for the aorta and para-aortic glands and common femoral vessels.
If a swelling is palpable, spend time eliciting its features.
Palpate both groins.
Examine the external genitalia
40.
LEFT KIDNEY
• Theright hand is placed anteriorly in the left lumbar region while the
left hand is placed posteriorly in the left loin
• Ask the patient to take a deep breath in, press the left hand forward
and lift the right hand upward and inward
• The left kidney is not usually palpable unless either low in position or
enlarged
• Its lower pole, when palpable, is felt as a rounded firm swelling
between both right and left hands (i.e. bimanually palpable) and it can
be pushed from one hand to the other, in an action which is
called ‘ballotting’
41.
RIGHT KIDNEY
• Feelfor the right kidney in much the same way as for the left
• Place the right hand horizontally in the right lumbar region anteriorly
with the left hand placed posteriorly in the right loin Push forwards
with the left hand, lift the right hand inward and upward and ask the
patient to take a deep breath in
• The lower pole of the right kidney, unlike the left, is commonly
palpable in thin patients and is felt as a smooth, rounded swelling
which descends on inspiration and is bimanually palpable and may be
‘balloted’ (bounced back and forth between the two examining
hands).
42.
SPLEEN
• Like theleft kidney, the spleen is not normally palpable
• It has to be enlarged to two or three times its usual size before it
becomes palpable and then is felt beneath the left subcostal margin
• Enlargement takes place in a superior and posterior direction before it
becomes palpable subcostally
• Once the spleen has become palpable, the direction of further
enlargement is downwards and towards the right iliac fossa
43.
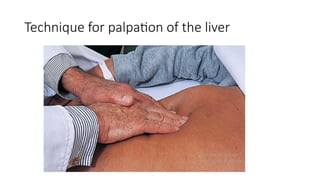
LIVER
• Sit onthe couch beside the patient. Place both hands side by side flat
on the abdomen in the right subcostal region lateral to the rectus,
with the fingers pointing towards the ribs.
• If resistance is encountered, move the hands further down until this
resistance disappears.
• Exert gentle pressure and ask the patient to breathe in deeply.
Concentrate on whether the edge of the liver can be felt moving
downwards and under the examining hand
44.
Cont..
• The liveris often palpable in normal patients without being enlarged.
• The lower edge of the liver can be clarified by percussion as can the
upper border in order to determine overall size: a palpable liver edge
can be due to enlargement or to displacement downwards by lung
pathology
• Hepatomegaly is conventionally measured in centimeters palpable
below the right costal margin, which should be determined with a
ruler if possible.
The urinary bladder
•Normally the urinary bladder is not palpable
• When it is full and the patient cannot empty it (retention of urine), a
smooth, firm, regular oval-shaped swelling will be palpated in the
suprapubic region and its dome (upper border) may reach as far as
the umbilicus
47.
Cont..
• What todo when an abdominal mass is palpable
• Describe its:
a. Site
b. Size and shape
c. Surface, edge and consistency
d. Mobility and attachments
48.
THE ANUS ANDRECTUM
• The left lateral position is best for routine examination of the rectum
• Make sure that the buttocks project over the side of the couch with
the knees drawn well up and that a good light is available
• Put on disposable gloves and stand behind the patient’s back, facing
the patient’s feet
• Explain to the patient what you are about to do, that you will be as
gentle as possible and that you will stop the examination if requested,
at any time
49.
Inspection
• Separate thebuttocks carefully and inspect the perianal area and
anus
• Note the presence of any abnormality of the perianal skin, such as
inflammation, warts, anal fissures, hemorrhoids, fistula etc
50.
Digital rectal examination(palpation)
• Put a generous amount of lubricant on the gloved index finger of the
right hand, place the pad of the finger (not the tip) flat on the anus
and press firmly and slowly (flexing the finger) in a slightly backwards
direction
• Feel for any thickening or irregularity of the wall of the canal, making
sure that the finger is carefully turned through a full circle (180° each
way)
• Assess the tone of the anal musculature; it should normally grip the
finger firmly. If there is any doubt, ask the patient to contract the anus
on the examining finger
51.
Cont..
• With experienceit is usually possible to feel a shallow groove just
inside the anal canal which marks the dividing line between the
external and internal sphincter
• The anorectal ring may be felt as a stout band of muscle surrounding
the junction between the anal canal and rectum
• Now pass the finger into the rectum, assess for the prostate gland
• It forms a rubbery, firm swelling about the size of a large walnut. Run
the finger over each lateral lobe, which should be smooth and regular.
Between the two lobes lies the median sulcus, which is palpable as a
faint depression running vertically between each lateral lobe.
52.
Cont..
• On withdrawingthe finger after rectal examination, look at it for
evidence of mucus, pus and blood, either fresh or altered
• If in doubt, wipe the finger on a white swab