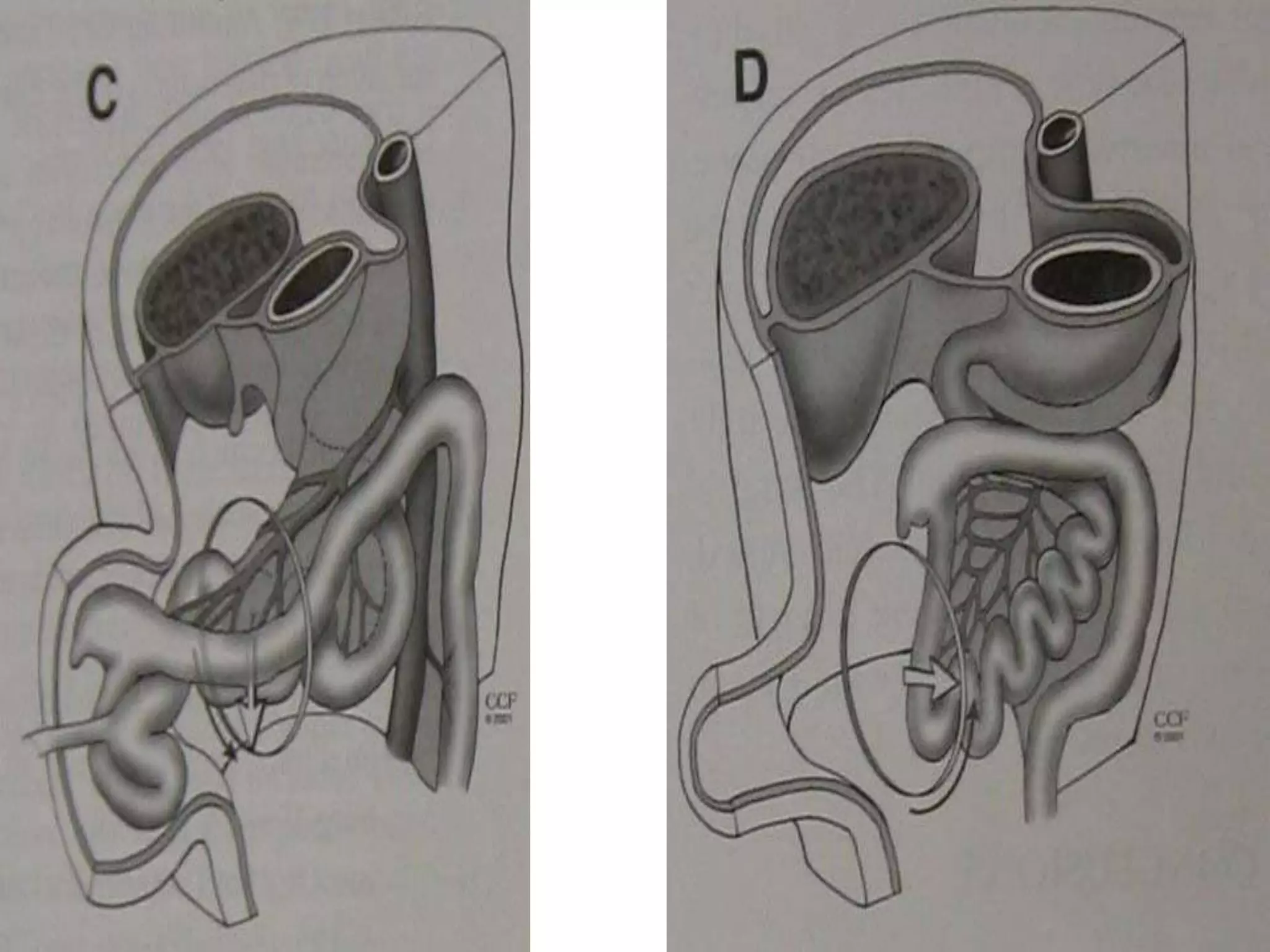
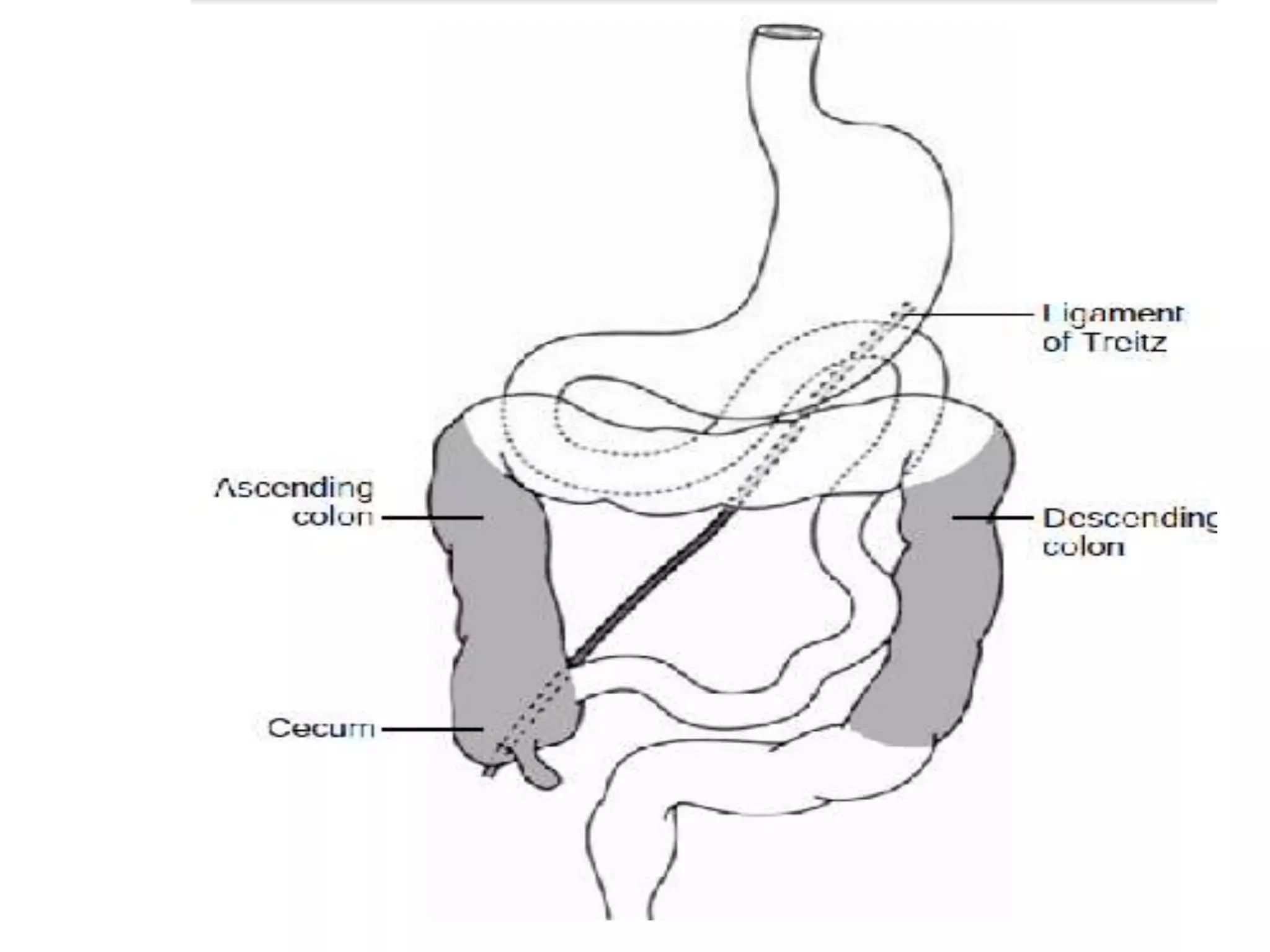
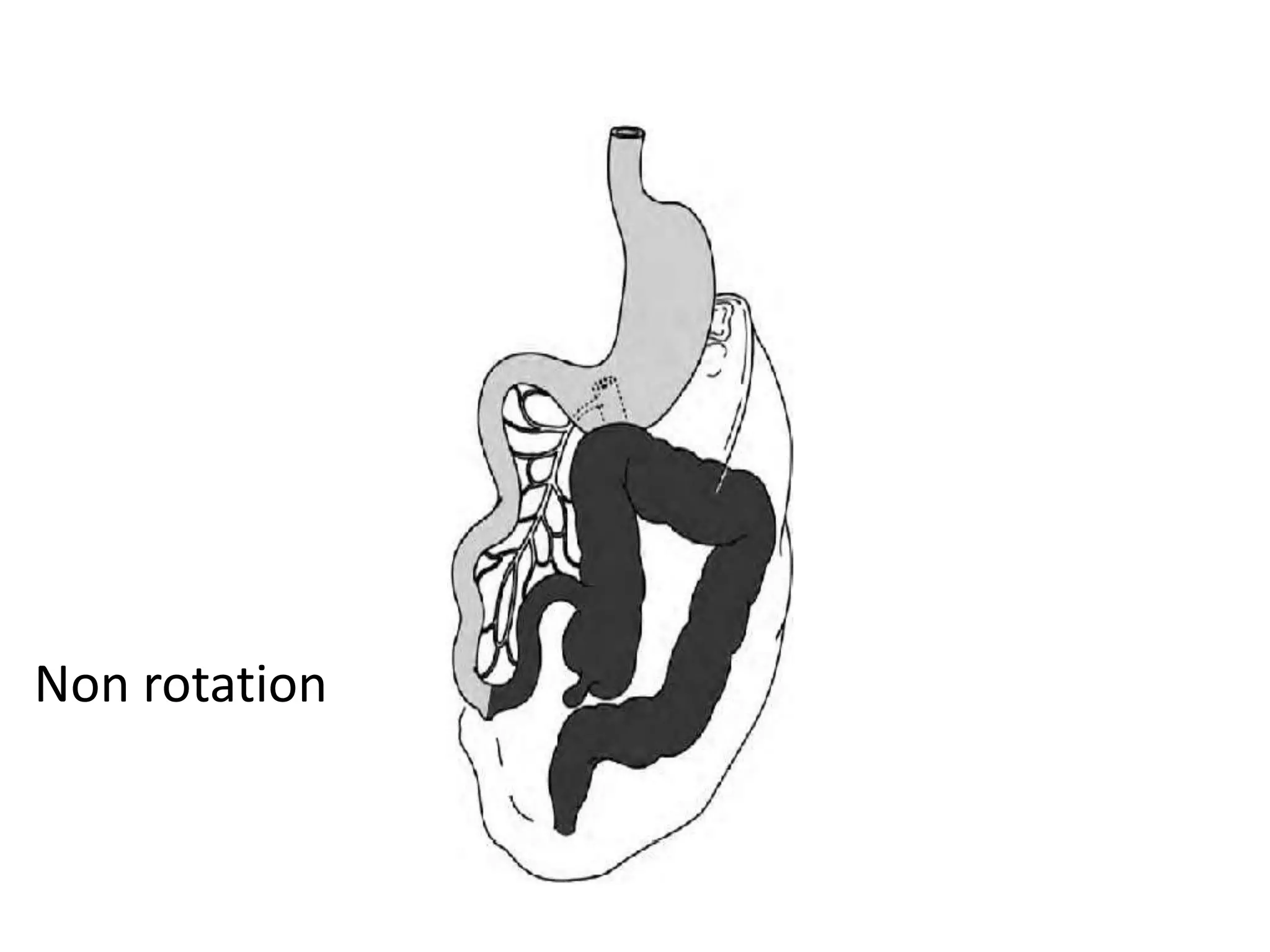
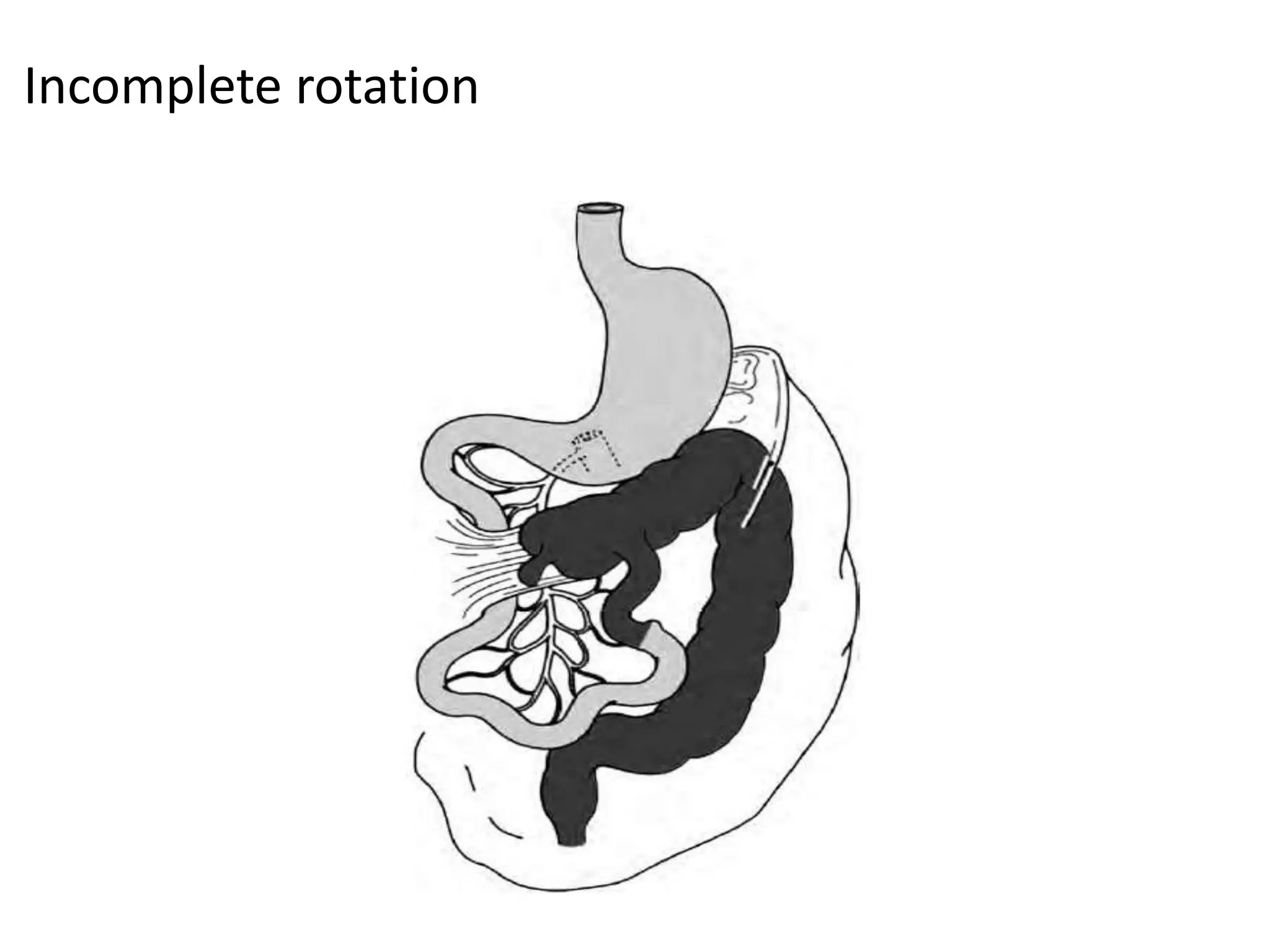
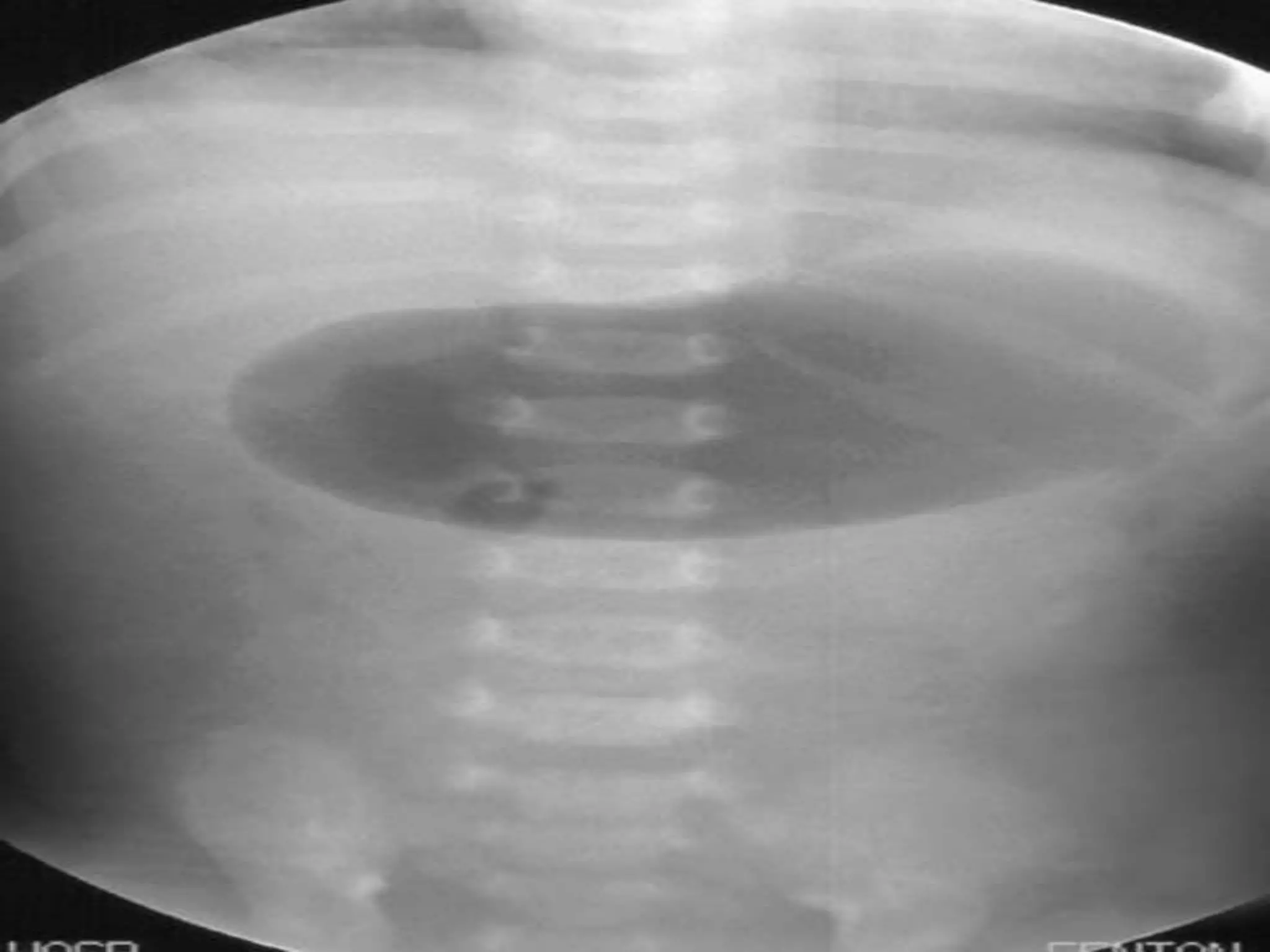
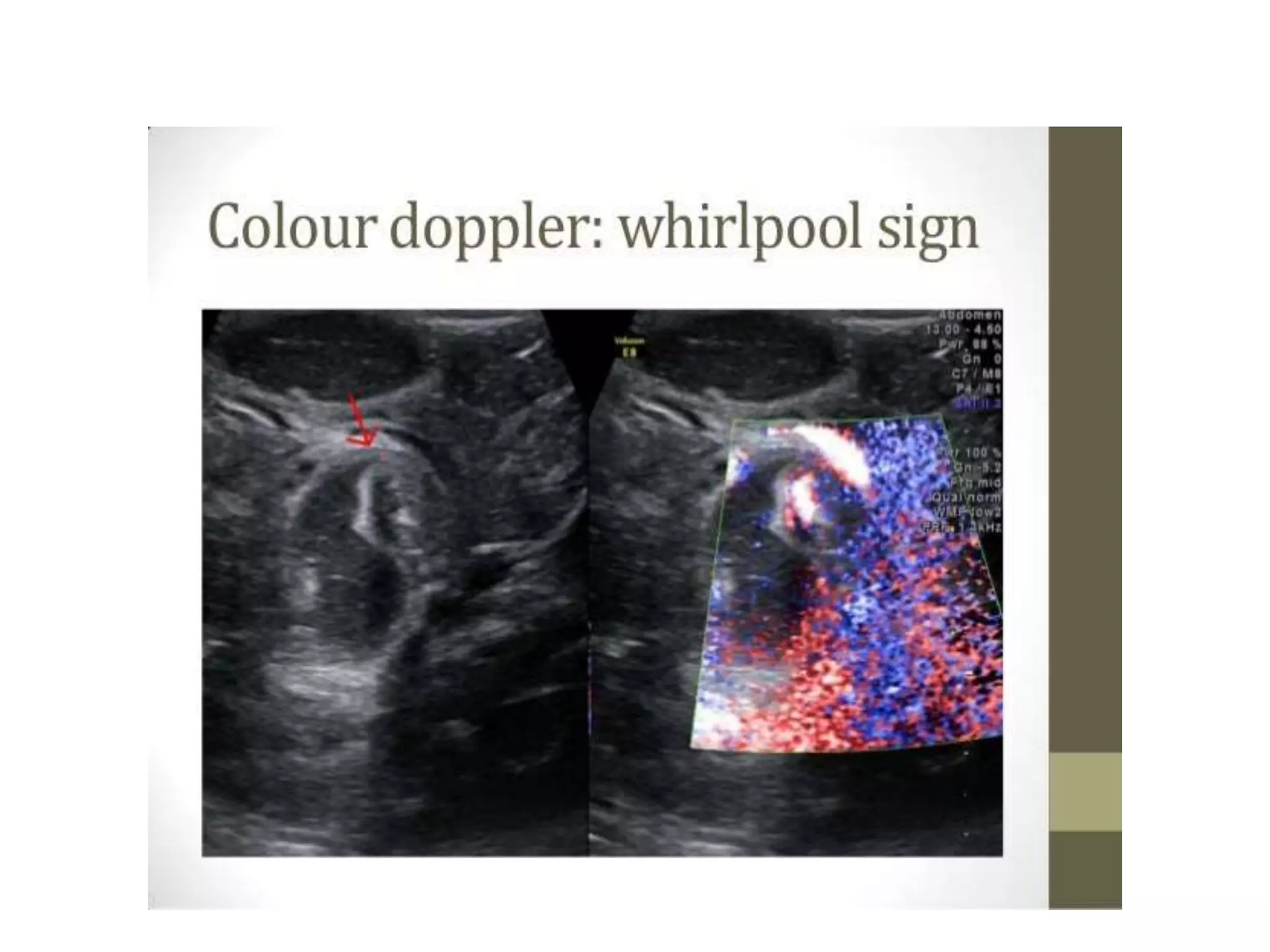
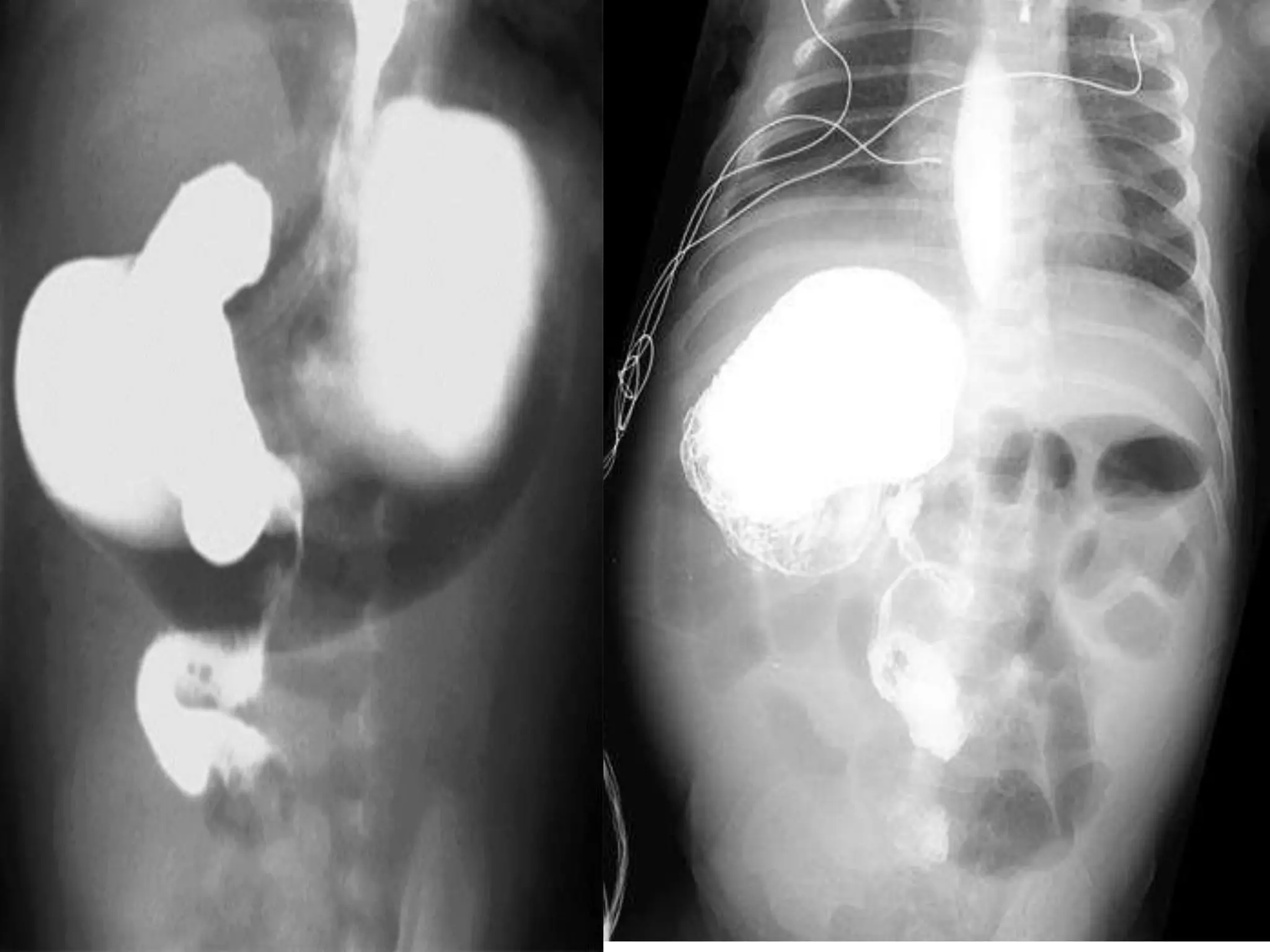
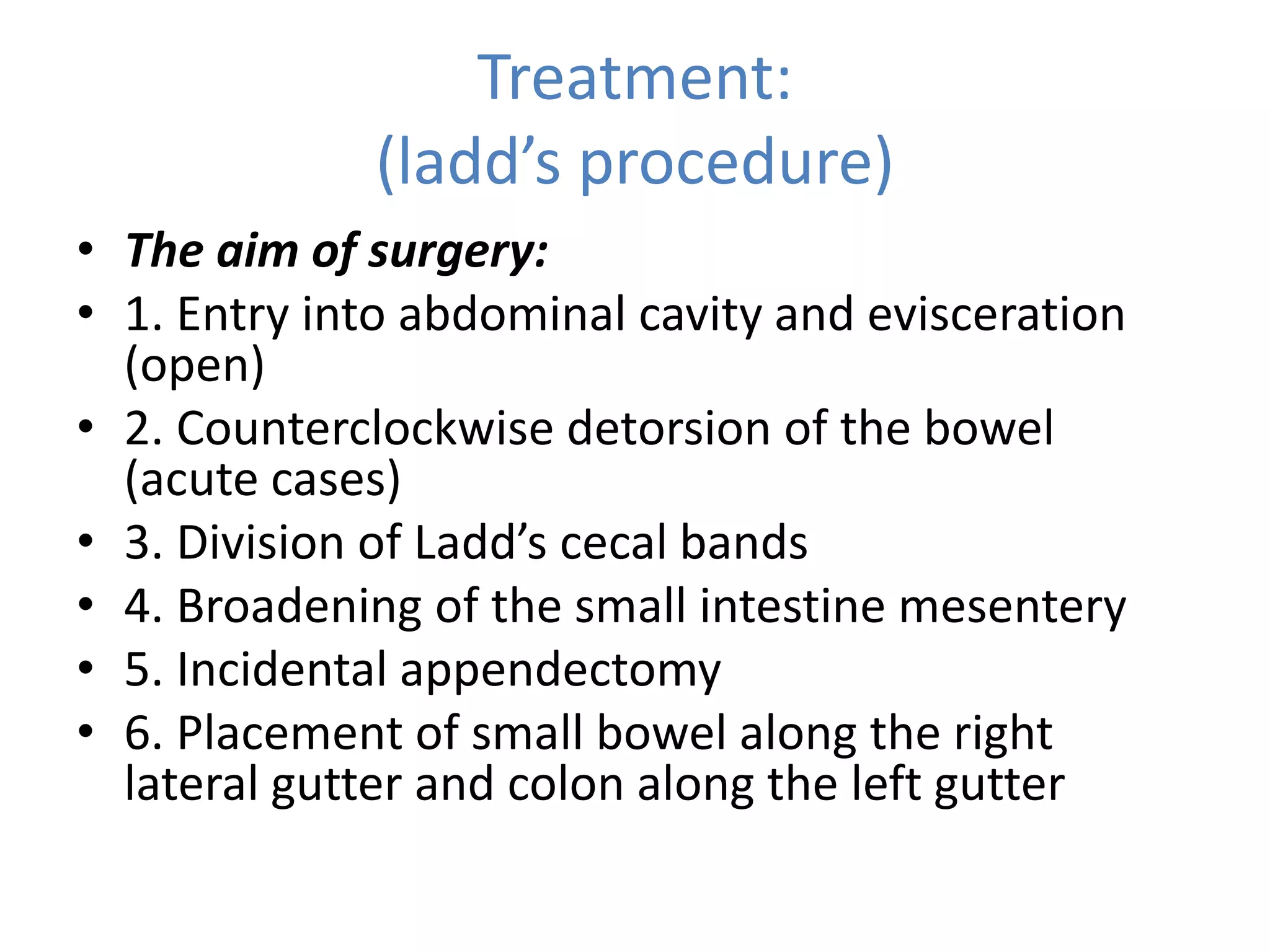
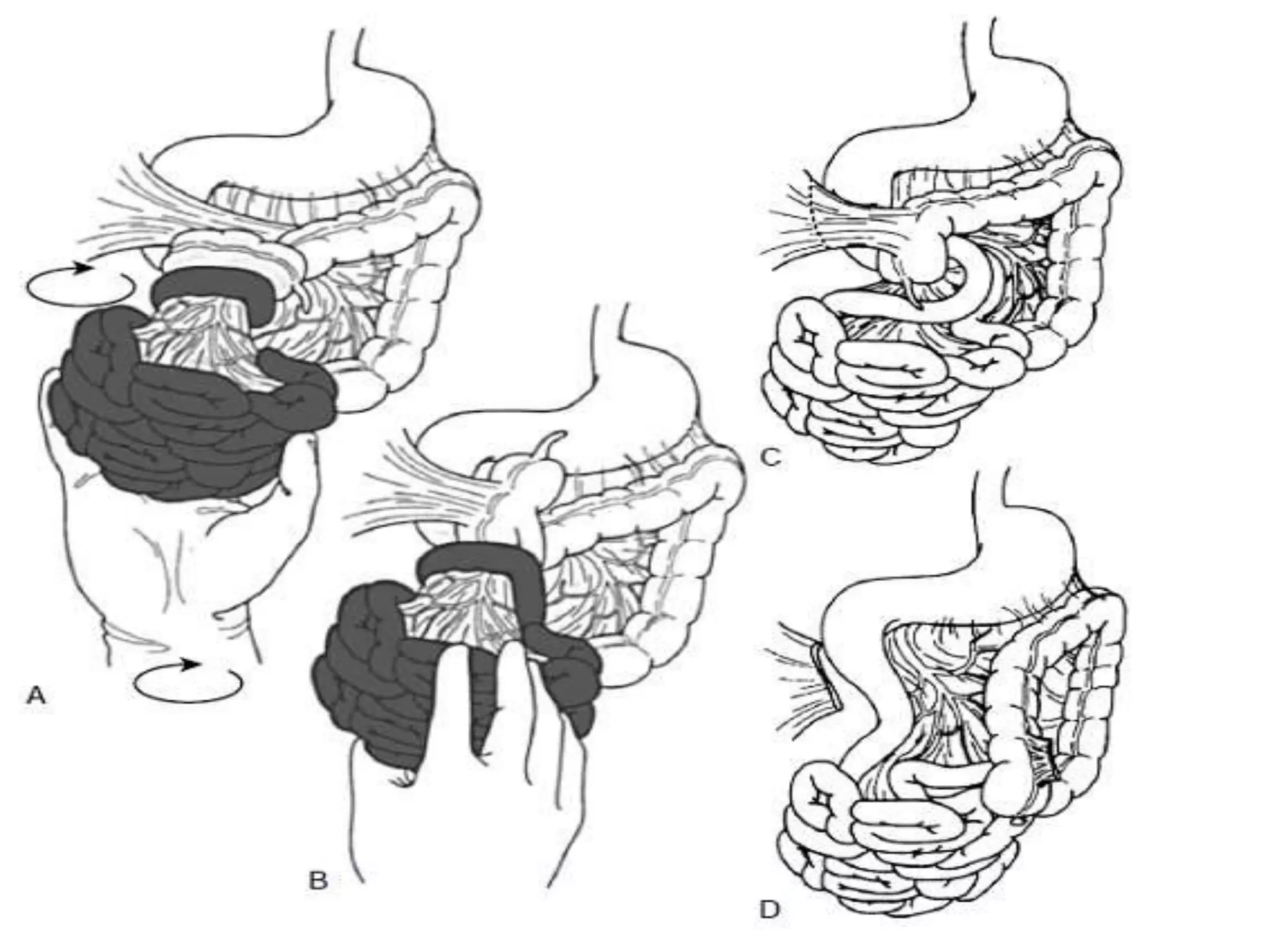
This document discusses malrotation, a condition that results from abnormal rotation of the embryonic gut. Malrotation can present at any age, but most commonly in infants under 1 month old, with bilious vomiting being the main symptom. The diagnosis is made through imaging studies like ultrasound or CT scan. Treatment involves surgery to untwist the bowel (Ladd's procedure), divide bands, and position the intestines in the correct locations to prevent future twisting. Early diagnosis and surgical intervention are important to reduce risks of complications like intestinal gangrene.