Download as PDF, PPTX

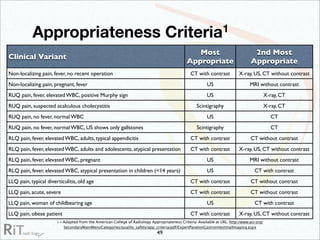

The document discusses the imaging modalities used in evaluating acute abdominal pain, including radiography, ultrasound, computed tomography (CT), and scintigraphy, highlighting their roles, indications, and limitations. It emphasizes the complexity of diagnosing acute abdomen due to its broad differential diagnoses and the necessity for accurate imaging to inform timely management. Additionally, the document outlines considerations such as patient history, contrast medium reactions, and appropriate imaging criteria based on various clinical presentations.