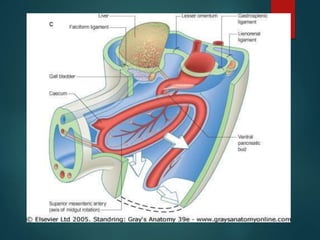
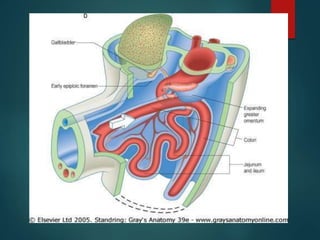
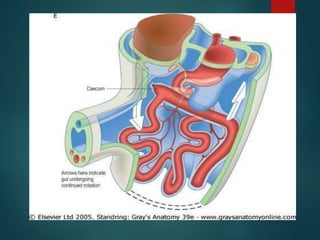
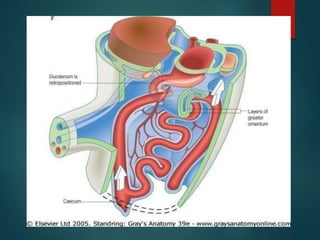
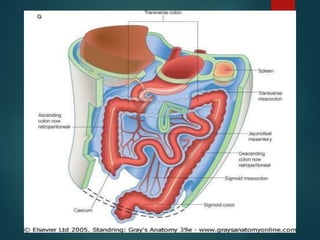
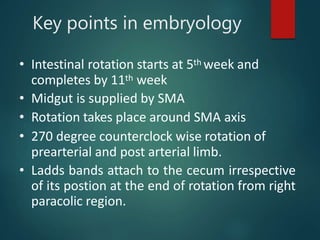
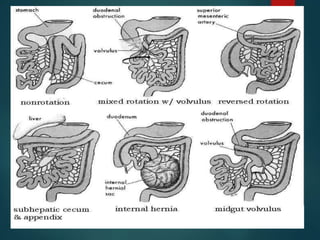
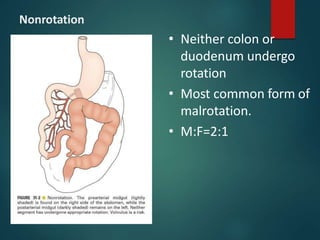
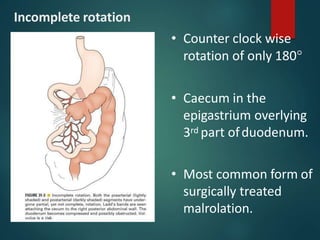
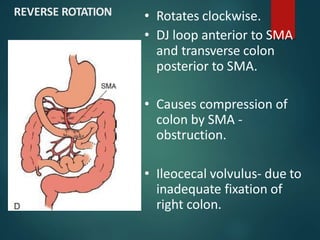
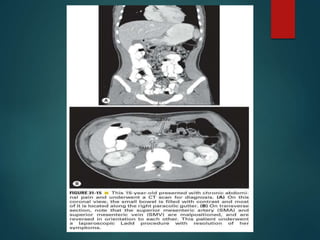
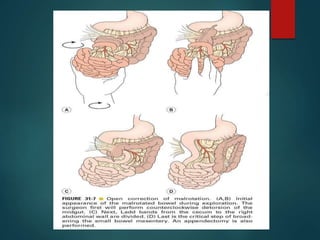
This document discusses intestinal malrotation, which occurs due to abnormal intestinal rotation and fixation during development. It describes the normal stages of intestinal rotation and fixation. Rotational disorders include nonrotation, incomplete rotation, and reverse rotation. Clinical manifestations include acute midgut volvulus in infants and chronic symptoms in older children. Radiologic imaging plays a key role in diagnosis. Treatment involves reducing recurrence of volvulus through the Ladd's procedure to divide abnormal bands and fix the intestine in normal positions.

![References
• Pediatric surgery. —7th ed. / editor in chief,
Arnold G. Coran ; associate editors, N. Scott
Adzick . . [et al.]
• Ashcraft’s pediatric surgery / [edited by]
George Whitfield Holcomb III, J. Patrick
Murphy ; associate editor, Daniel J. Ostlie. —
5th ed.](https://image.slidesharecdn.com/malrotation-210511123819/85/Malrotation-49-320.jpg)