Downloaded 11 times







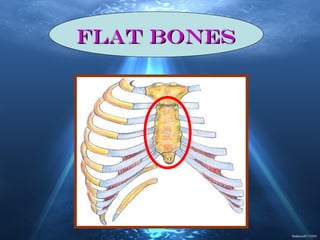


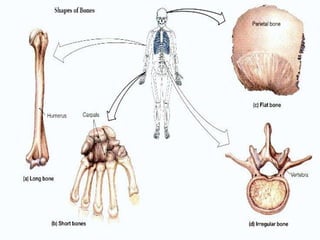









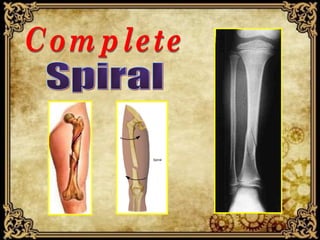



















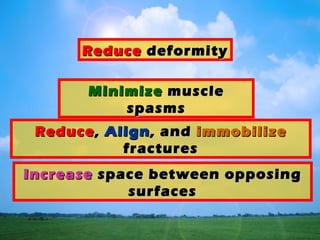






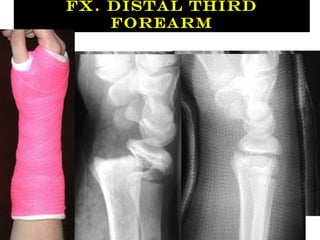
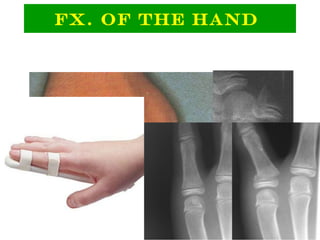







This document discusses orthopedic fractures and their treatment. It describes different types of bones and people who are prone to fractures. Fractures can be closed or open, displaced or non-displaced. The key principles of fracture management are to splint the bone above and below the fracture, loosely cover any open wounds, assess neurovascular function, and apply gentle traction to long bones to maintain alignment. Early management focuses on splinting, minimizing muscle spasms, reducing, aligning and immobilizing fractures, and monitoring the patient.




































































































