Downloaded 18 times

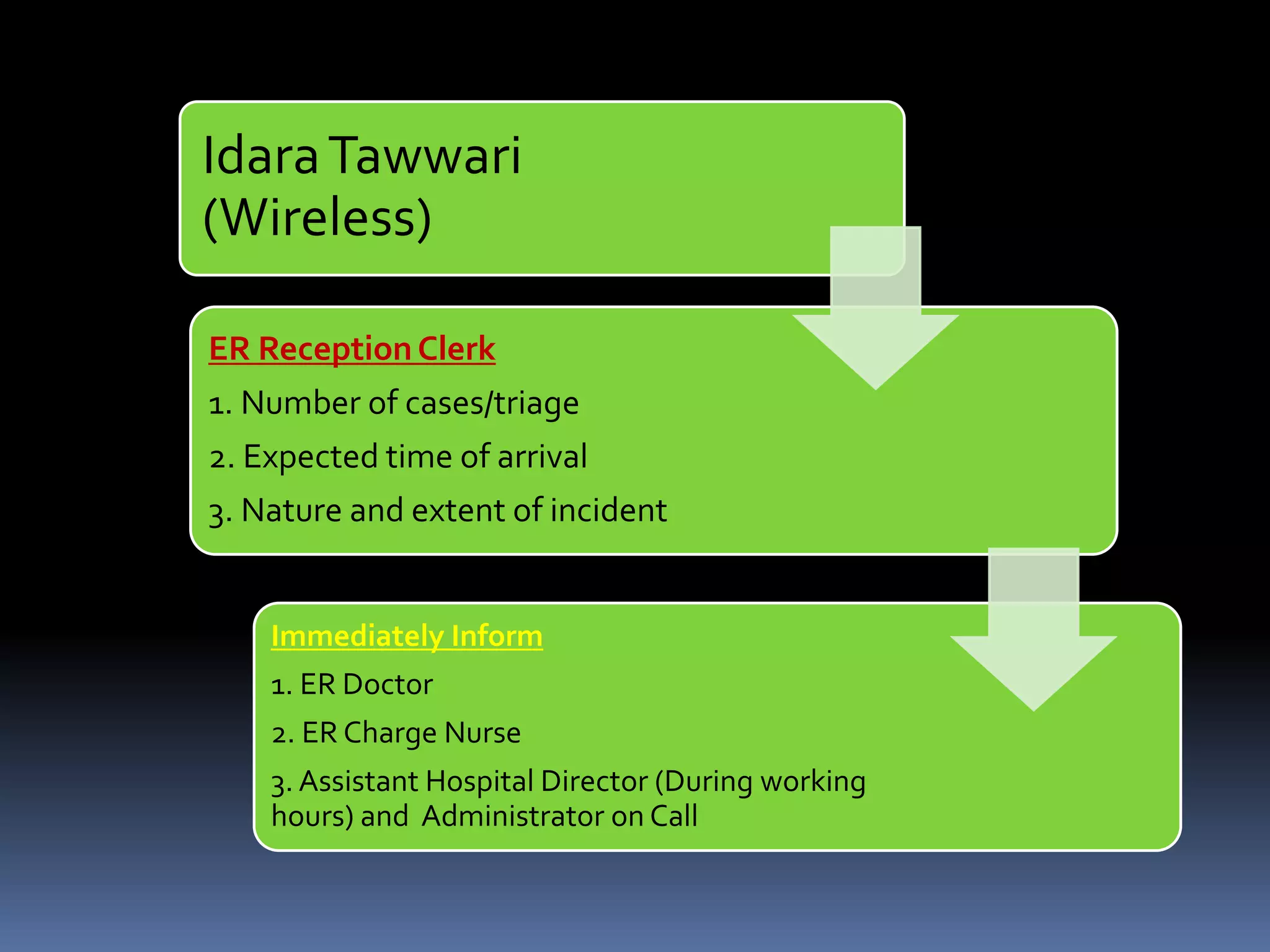
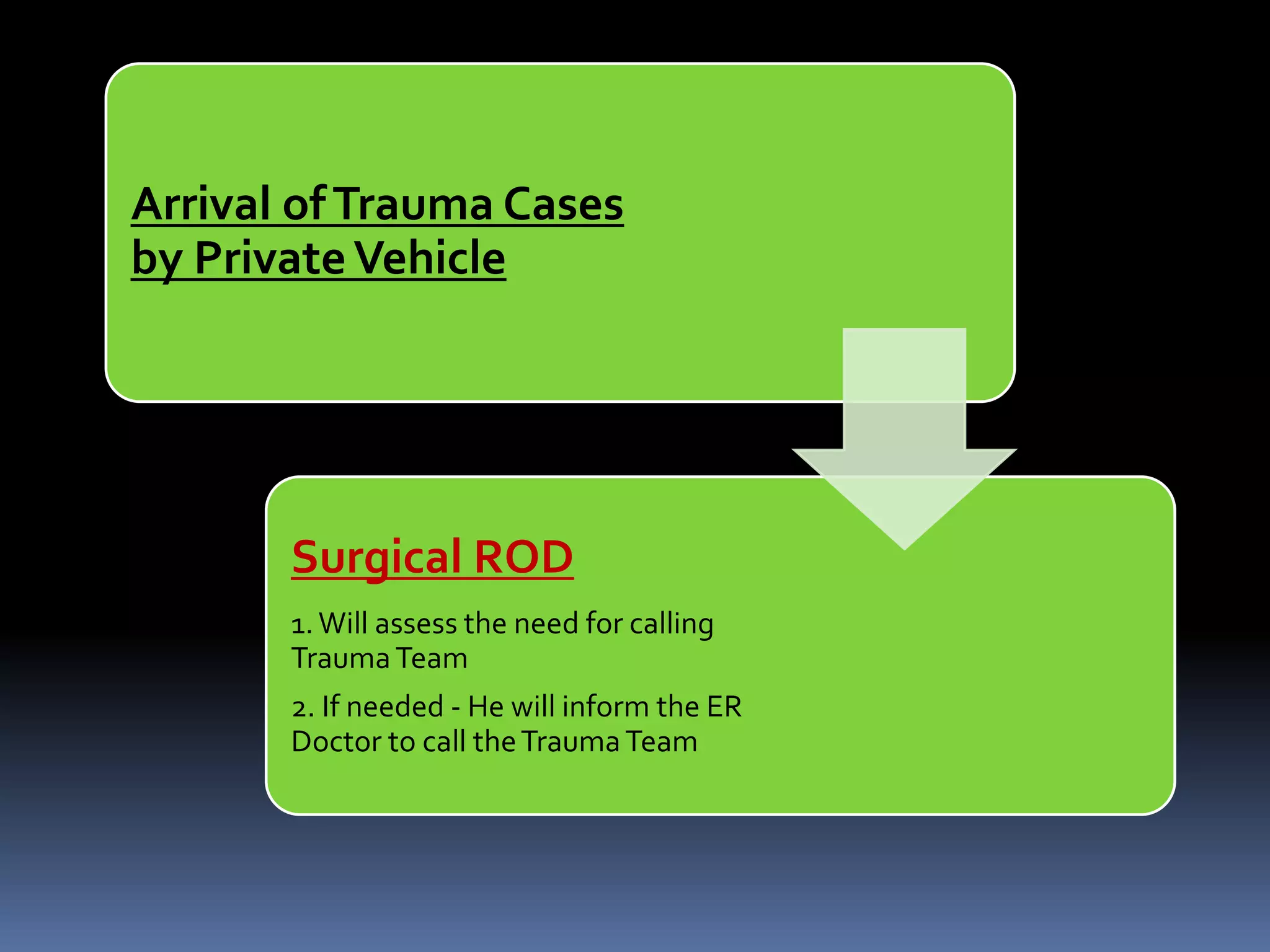
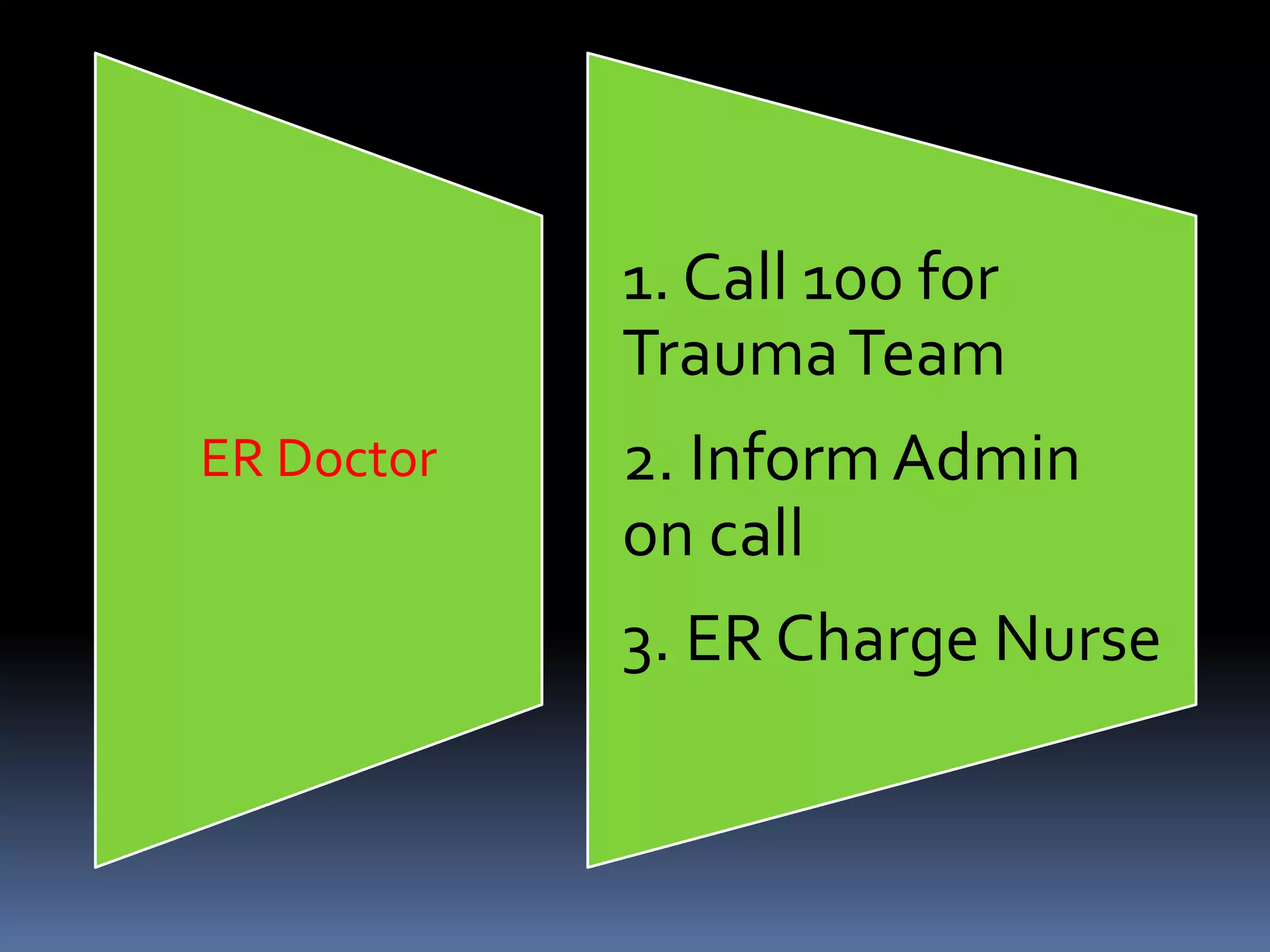






This document outlines the trauma team policy for a hospital's Patient Safety Department. It establishes the first trauma team policy with an implementation date of January 1, 2016. The purpose is to decrease mortality and morbidity from acute trauma cases through timely coordinated action of various clinical and non-clinical teams. The policy defines the criteria for activating the trauma team, which includes severe trauma cases received through emergency services or referred from other hospitals. It also establishes the roles and responsibilities of the core clinical team, supporting clinical staff, and non-clinical coordinators who will respond to trauma activations.
















































































