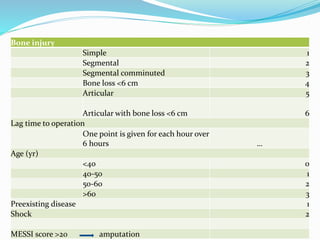
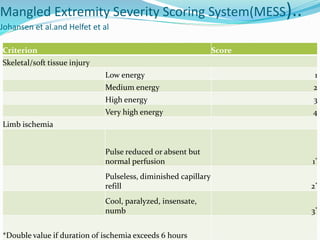
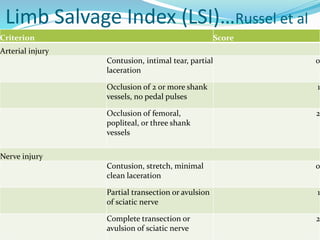
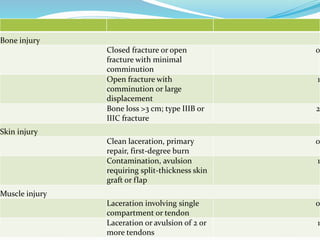
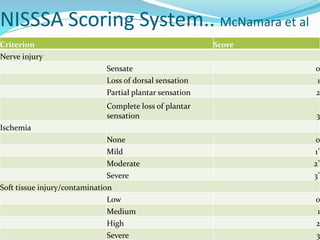
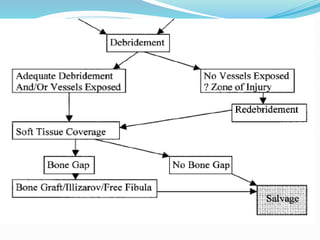
The document discusses mangled extremity injuries, which involve severe soft tissue, bone, vascular and nerve injuries to an extremity. It describes various scoring systems used to evaluate factors like ischemia time, bone/soft tissue damage, and patient characteristics to determine likelihood of successful limb salvage versus requiring amputation. The initial management of a mangled extremity involves stabilization, debridement of non-viable tissue, and restoration of vascular flow. Further treatments may include skeletal stabilization, soft tissue coverage using flaps/grafts, nerve repair, and hyperbaric oxygen to aid healing. Scoring systems guide but do not determine the decision between salvage and amputation.































































































![[TRAUMATOLOGY] SOFT TISSUE MANAGEMENT AND RECONSTRUCTION IN ORTHOPAEDICS EMER...](https://cdn.slidesharecdn.com/ss_thumbnails/softtissuemanagementandreconstraction-210729080619-thumbnail.jpg?width=640&height=640&fit=bounds)



























