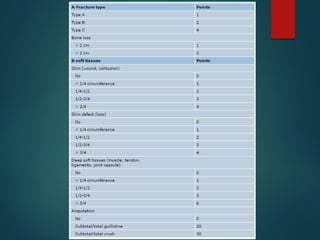
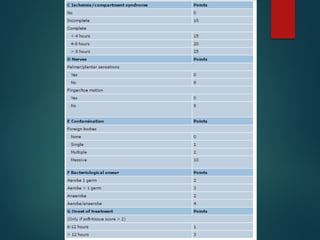
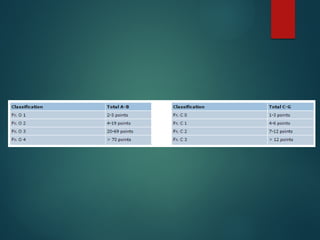
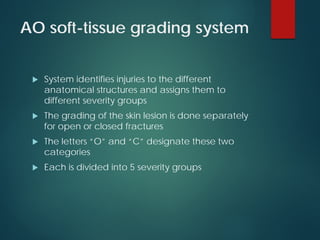
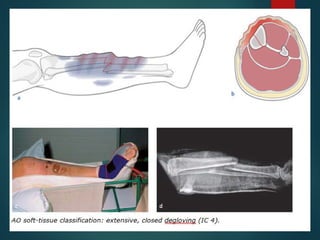
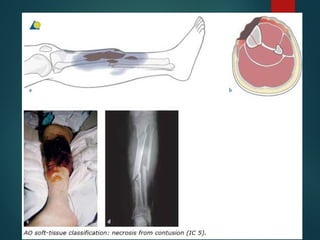
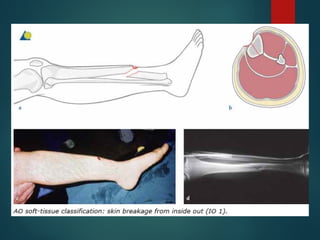
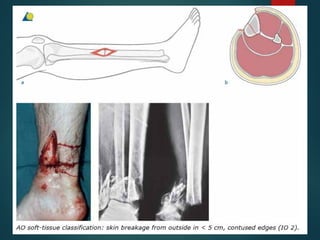
This document discusses different types of soft tissue injuries and classifications systems used to categorize them. It describes closed wounds like contusions and hematomas versus open wounds. Classification systems like Gustilo and Tscherne grade soft tissue damage and help determine appropriate treatment and prognosis. The goal is to effectively communicate injury severity and anticipate complications to improve patient outcomes.














![SOFT TISSUE INJURY [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofsofttissueinjuryrecovered-220424142623-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![[TRAUMATOLOGY] SOFT TISSUE MANAGEMENT AND RECONSTRUCTION IN ORTHOPAEDICS EMER...](https://cdn.slidesharecdn.com/ss_thumbnails/softtissuemanagementandreconstraction-210729080619-thumbnail.jpg?width=640&height=640&fit=bounds)









































