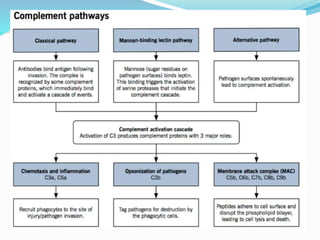
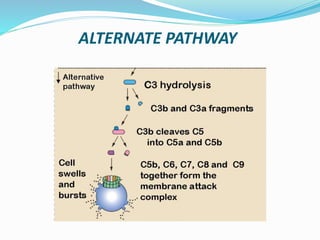
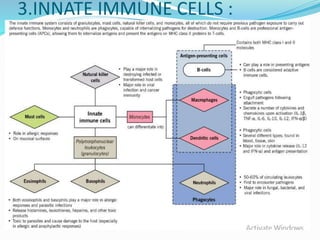
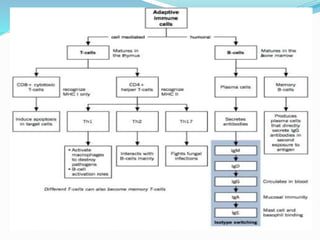
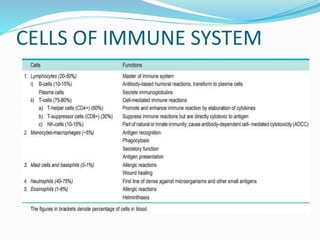
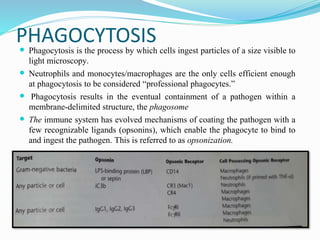
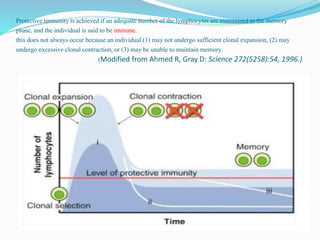
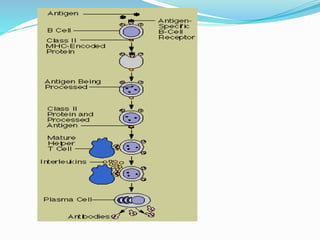
This document provides an overview of the immune system. It begins with definitions of immunity and the historical views of disease. It then describes the innate and adaptive immune systems in detail. The innate system includes physical barriers and the complement system. Adaptive immunity involves both humoral immunity through B cells and antibodies, and cell-mediated immunity through T cell subsets. Key immune cells like macrophages and neutrophils are also summarized in terms of their functions, including phagocytosis, antigen presentation, and cytokine secretion. The document provides an extensive but concise review of immune system components and their roles in protection from pathogens.