Downloaded 112 times
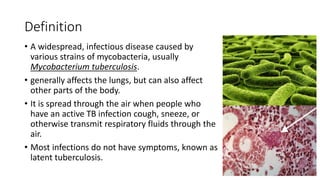







The document discusses tuberculosis (TB) in children, defining it as a prevalent infectious disease primarily affecting the lungs and transmitted through the air. It highlights the epidemiology, clinical manifestations, diagnostic tools, treatment protocols, and prevention strategies for TB in the pediatric population, emphasizing the importance of early detection and management. Additionally, it addresses drug-resistant TB and specific treatment regimens for various forms of the disease.























































































