● This isan acute generalized infection of the
intestinal lymphoid tissue,
gall-bladder and
reticuloendothelial system.
• It includes typhoid fever which affects 90% of the
cases and paratyphoid which affects 10% of the
cases.
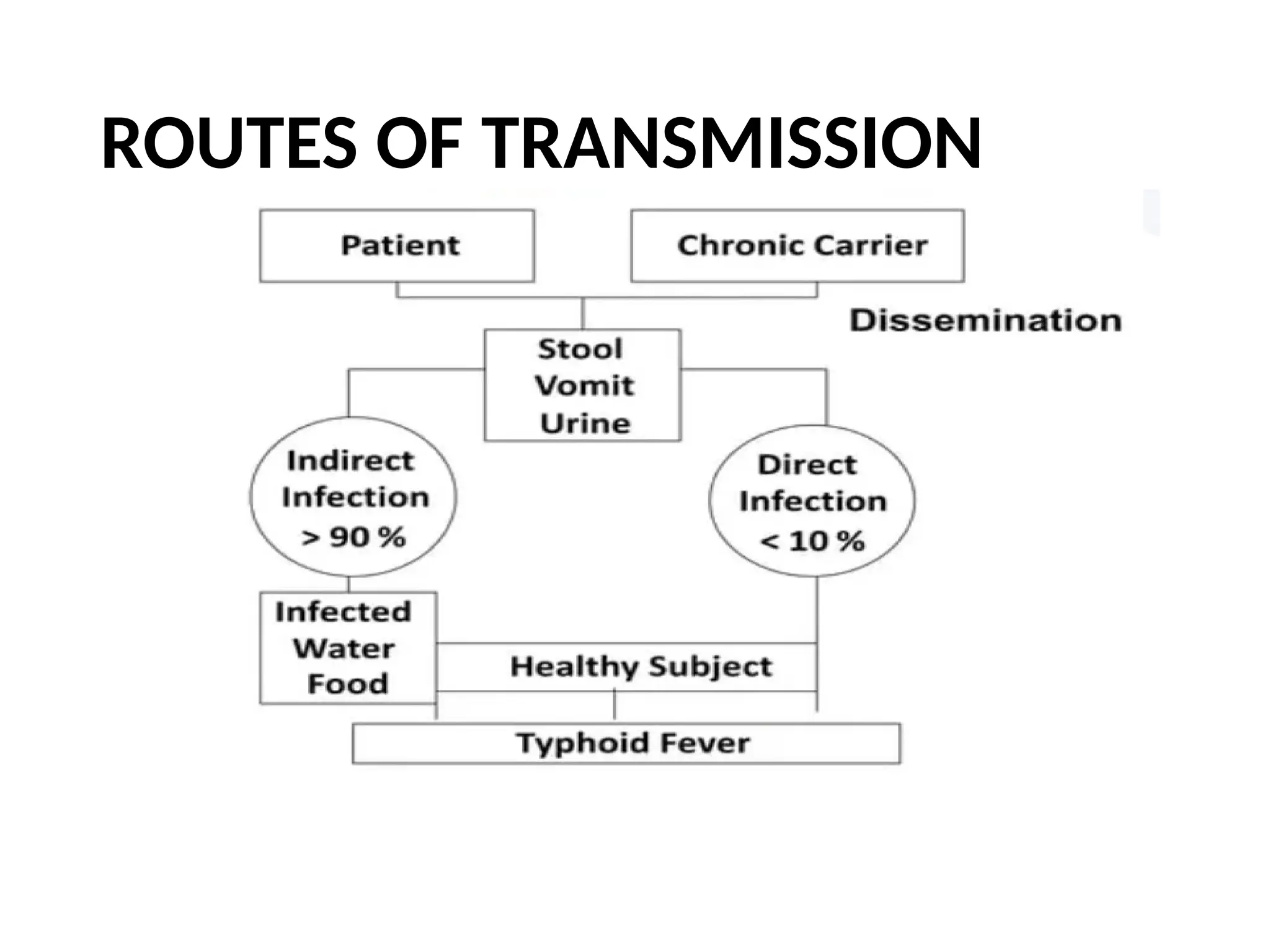
• Transmission is fecal oral.
INTRODUCTION.
3.
• Recent large-scaledata and modelling efforts estimate that
14.3 million cases of typhoid and paratyphoid fevers occurred
globally in 2017, a decline from 25.9 million cases in 1990.
• Incidence rates peak in the 5 to 9-year-old age-group, with
roughly 13% of cases occurring in children younger than 5
years and roughly 56% of cases among children younger than
15 years of age
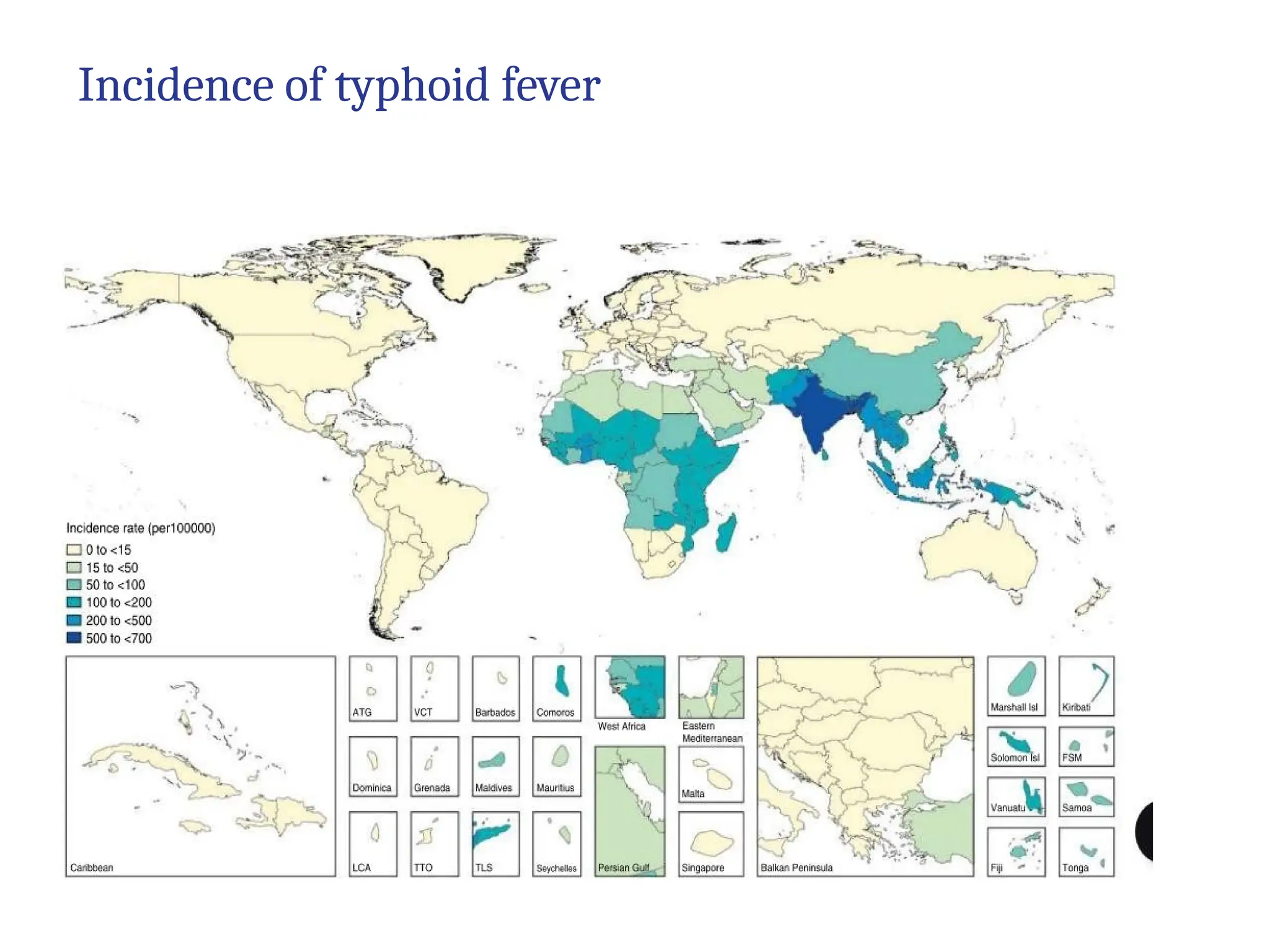
• South and Southeast Asia have notably high incidence rates,
whereas moderate incidence rates are reported from Central
and South America, Africa, Central and East Asia, and
Oceania.
• Disease occurs exclusively in human
EPIDEMIOLOGY
AGENT-
• Salmonella typhi–majorcause
• S.paratyphi A , B and C
• Family- Enterobactericeae
• Gram negative bacilli
• Motile with peritrichate flagella
• Non acid-fast
• Non capsulated
• Non spore forming
• Facultative anerobe
7.
The Enteric bacillihave 3 important
antigens:
✔O antigen (body or somatic)
• Less immunogenic
• Cross reacts
✔H antigen or flagellar antigen,
• Strongly anigenic
• Rapid rise of Ab in infection/immunisation
• Lasts longer and specific
✔Vi antigen (virulence antigen)
• S. Typhi and S.Paratyphi C
• Poorly immunogenic
• Disappears….. May persist in chronic carriers
9.
HOST
• Humans areonly reservoir and only known
susceptible host
• Peak incidence ---- 5 to 9 years.
• 10% of cases occur in infant age group.
• No sex predliction
• Children constitute 40-50% MDR typhoid cases with
higher case fatality rate
10.
• "Typhoid Mary"(MaryMallon) 1907- was the
first asymptomatic typhoid carrier to be identified by
medical science
Typhoid Mary in a 1909 newspaper illustration
11.
Environmental
Source of infection
❖Primary - faeces, urine of cases, carriers
❖ Secondary –
• contaminated water,
• food,
• fingers and
• flies.
12.
Spread of infecion
•Water contamination
• Food contamination
• Houseflies
Predisposing factors
• Over crowding
• Poor personal hygiene
• Poverty and illiteracy
• Poor sanitary and water supply suituations
• Open defecation
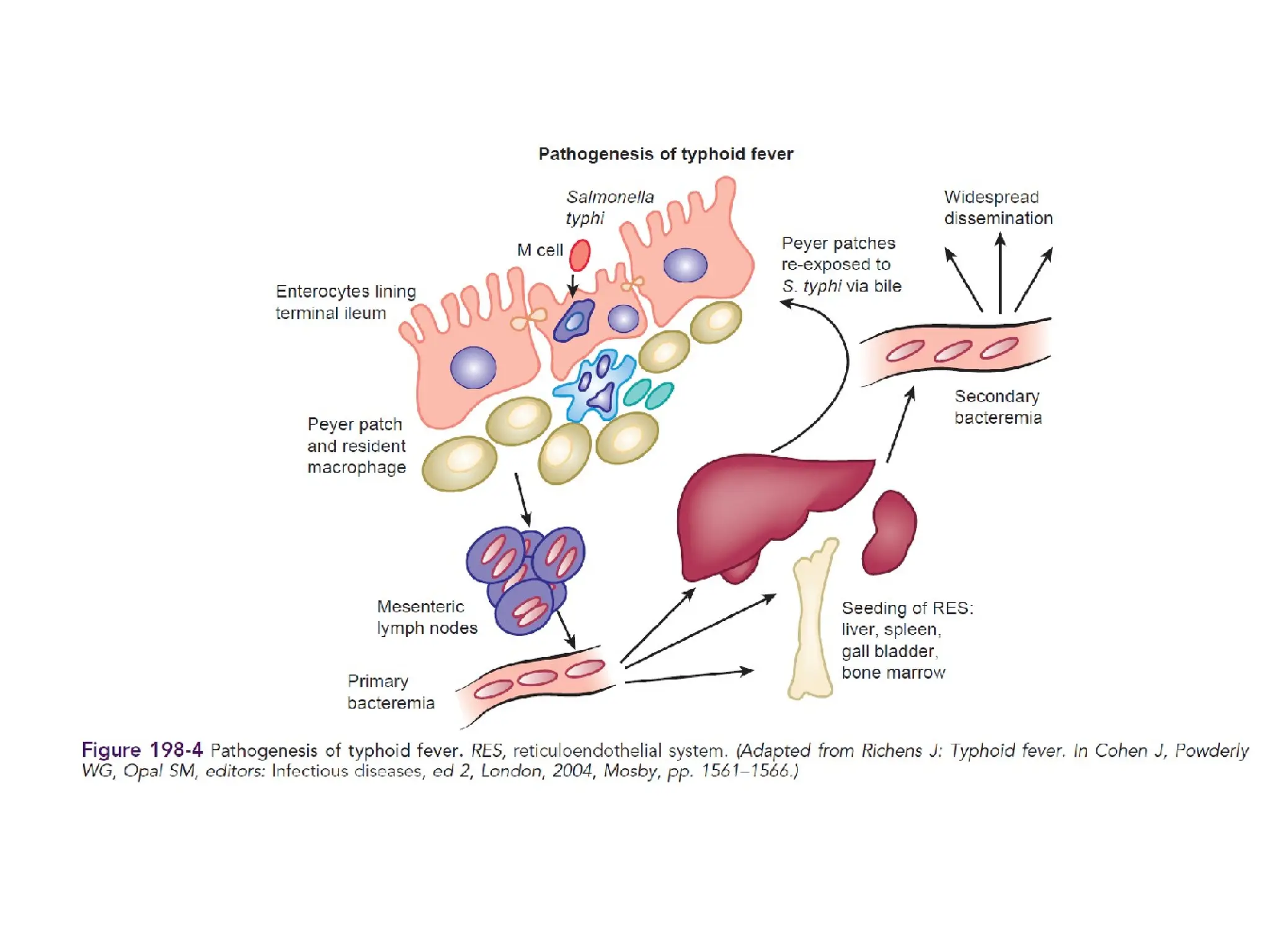
PATHOGENESIS
Ingestion
Invade body throughgut mucosa in terminal ileum.(possibly
through specialized antigen sampling cells known as M cells)
Pass through intestinal mucosa
S. Typhi enter mesenteric lymphoid system
Lymphatics
Bloodstream (Asymptomatic bacteremia, Culture negative)
Colonize Reticuloendothelial system (replicate in
macrophages)
Shed back into blood (Secondary bacteremia-Symptoms
18.
Virulence factors
• Genes– regulate invasion of Payer’s patches
• Inoculum size
▪ 25% for 105
▪ 50% for 107
▪ 75% for 109
• Gastric pH
• Vi polysaccharide antigen
• Concommitant H. Pylori infection/HIV infection
• Immunocompetence
19.
Clinical features
• Incubationperiod- 3 to 30 days – depending on
size of inoculum……(usually 7-14days)
• Symptoms occur in 1-2 weeks
• Clinical picture exhibits a wide range of clinical
severity and varies according to age
• Mild pyrexia ------------> fatal severe disease
20.
In neonates
▪ infectionis transmitted vertically
▪ Mother has chorioamnionitis- may lead to
abortion or premature delivery.
▪ Presents with
• Hypothermia or hyperthermia
• Vomiting
• Diarrhoea
• Abdominal distention
• Seizures
• Jaundice
• Hepatomegaly
• Failure to thrive
21.
In infants andchildren up to 5 years
• Disease may be mild
• Presenting only as diarrhea
• Or mimicking a viral illness
• The early stages of the disease may be very difficult to
differentiate from other endemic diseases, such as
malaria and dengue fever.
• In some cases, a macular or maculopapular rash (“rose
spots”) may be visible around the seventh to tenth day
of the illness.
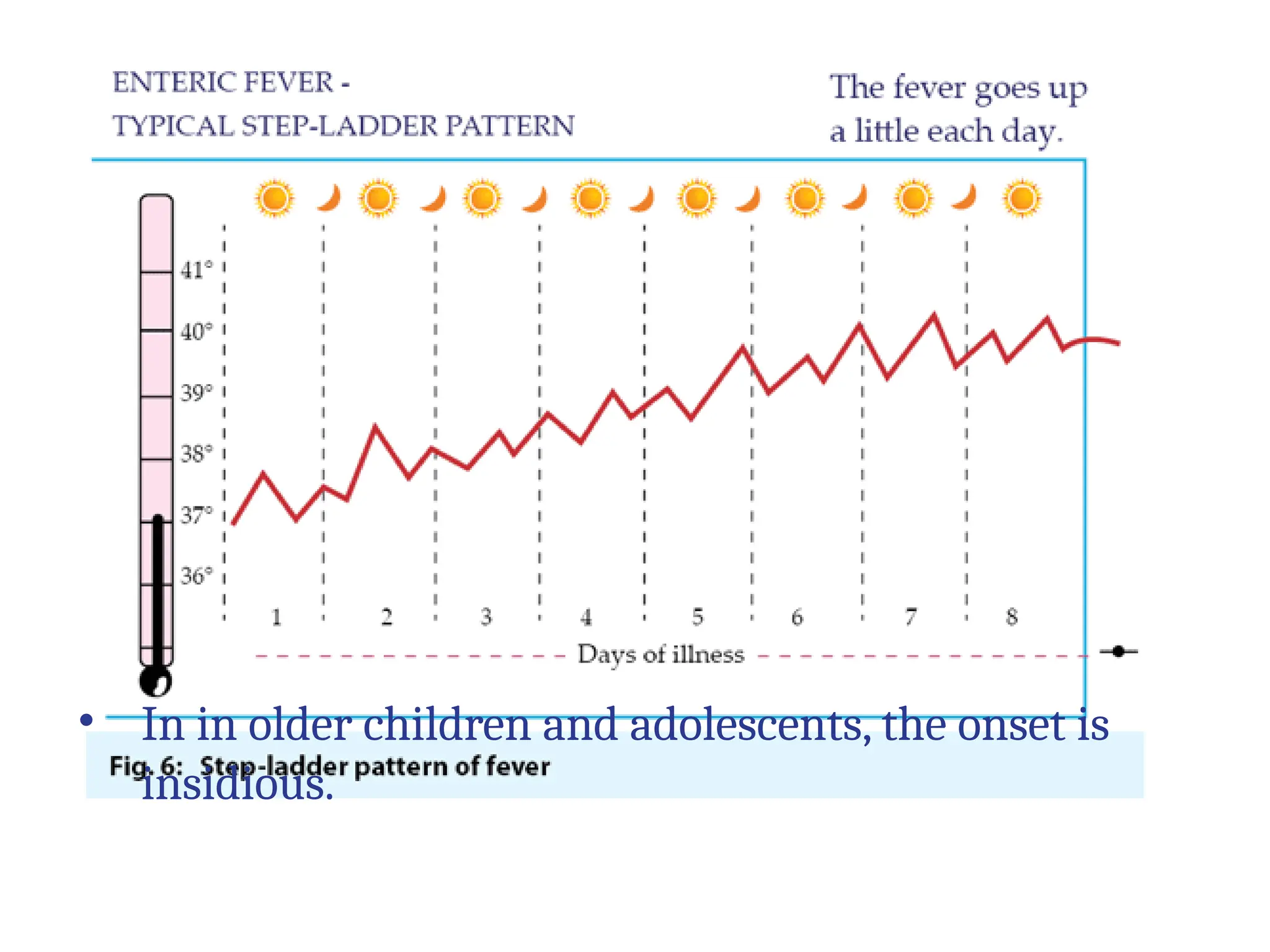
• In in older children and adolescents, the onset is
insidious.
22.
Initial symptoms –over2-3 days
• fever(95%)
• coated tongue(76%)
• anorexia(70%)
• Vomiting
• Hepatomegaly
• Splenomegaly
• diarrhoea
• malaise
• myalgia , headache
• abdominal pain
• Diarrhoea - constipation
• cough and epistaxis
• Severe lethargy
• Relative bradycardia seen in older children and
adults
23.
CLINICAL FEATURES
• Firstweek: malaise, headache, cough & sore throat in prodromal stage.
The disease classically presents with step-ladder fashion rise temperature
(40 - 41°C) over 4 to 5 days, accompanied by headache, vague abdominal
pain, and constipation or pea soup Diarrhoea.
• Second week: Between the 7th -10th day of illness, mild
hepatosplenomegally occurs in majority of patients. Relative bradycardia
may occur and rose-spots may be seen.
• Third week: The patient will appear in the "typhoid state" which is a state
of prolonged apathy, toxemia, delirium, disorientation and/or coma.
Diarrhoea will then become apparent. If left untreated by this time, there
is a high risk (5-10%) of intestinal hemorrhage and perforation.
• Rare complications: Hepatitis, Pneumonia, Thrombophlebitis,
Myocarditis, Cholecystitis, Nephritis, Osteomyelitis, and Psychosis. 2-5%
patients may become Gall-bladder carriers
24.
• In inolder children and adolescents, the onset is
insidious.
Hemorrhage and Perforation
•Intestinal haemorrhage (<1%) and perforation (0.5-1%)
are infrequent among children.
• Intestinal perforation may be preceded by a marked
increase in abdominal pain, tenderness, vomiting, and
features of peritonitis
Intestinal perforation and peritonitis may be accompanied by
• a sudden rise in pulse rate,
• hypotension,
• marked abdominal tenderness and guarding and
subsequent abdominal rigidity.
• A rising white blood cell count with a left shift and
• free air on abdominal radiographs
29.
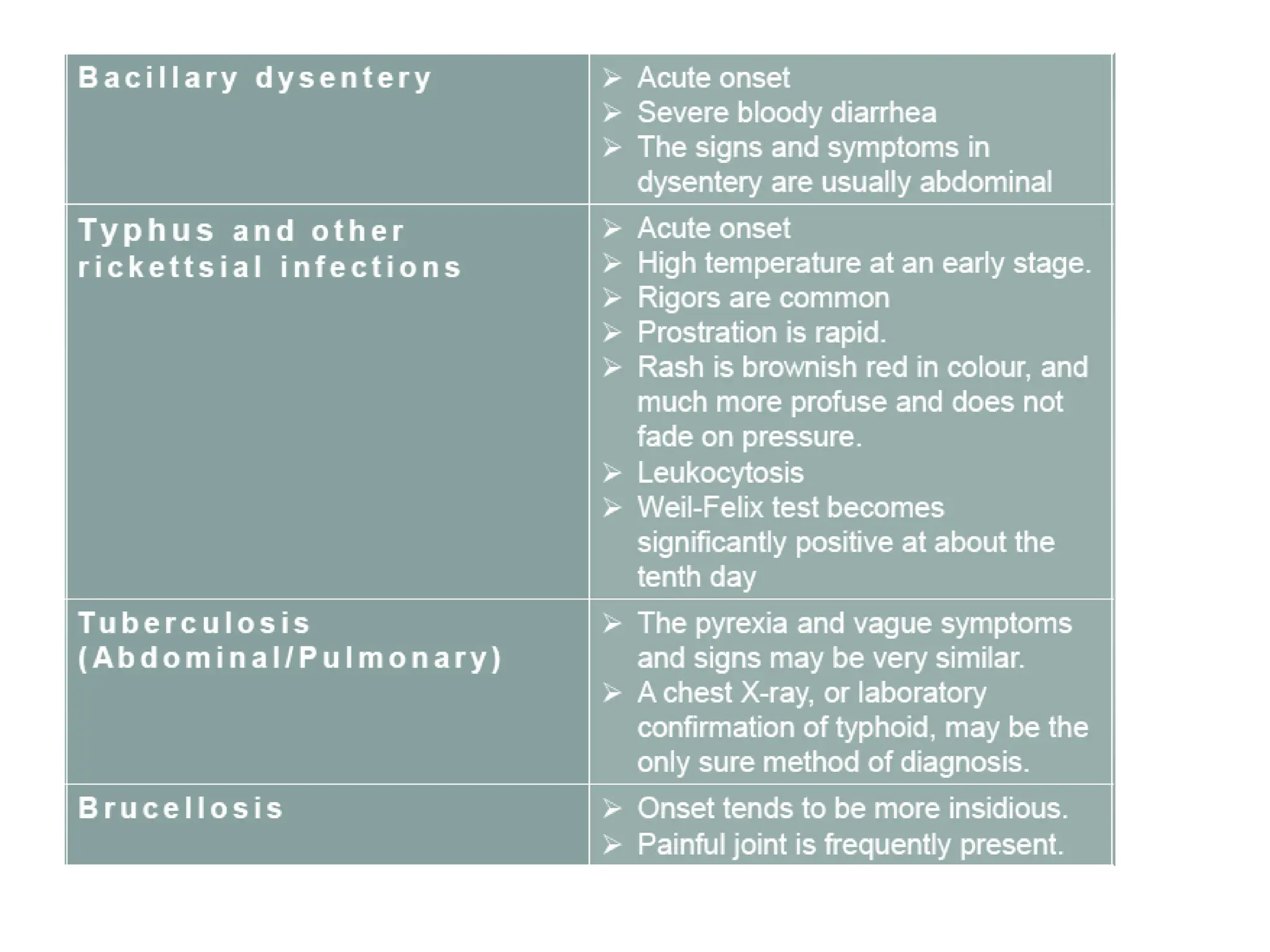
DIFFERENTIAL DIAGNOSIS
Salmonella infectionand gastroenteritis - Salmonellae,
The dysentery group may occasionally cause an invasive illness
resembling typhoid fever with bacteremia. however, the GIT Symptoms
are more acute than the general manifestations, and the pyrexia much
lower and of shorter duration.
Lab investigations..
Complete bloodcount
Hb-normal.
Severe anaemia is unusual if present should suspect Intestinal
haemorrhage
WBC Count-normal
TC –Leukopenia seen in 20-25%cases.
DC-Neutrophilia and Eosinopenia present in 70-80%cases.
PLC- normal. Thrombocytopenia marker of severe ileus, DIC
Mild elevation transaminases 2-3 times (SGOT>SGPT) May be seen
34.
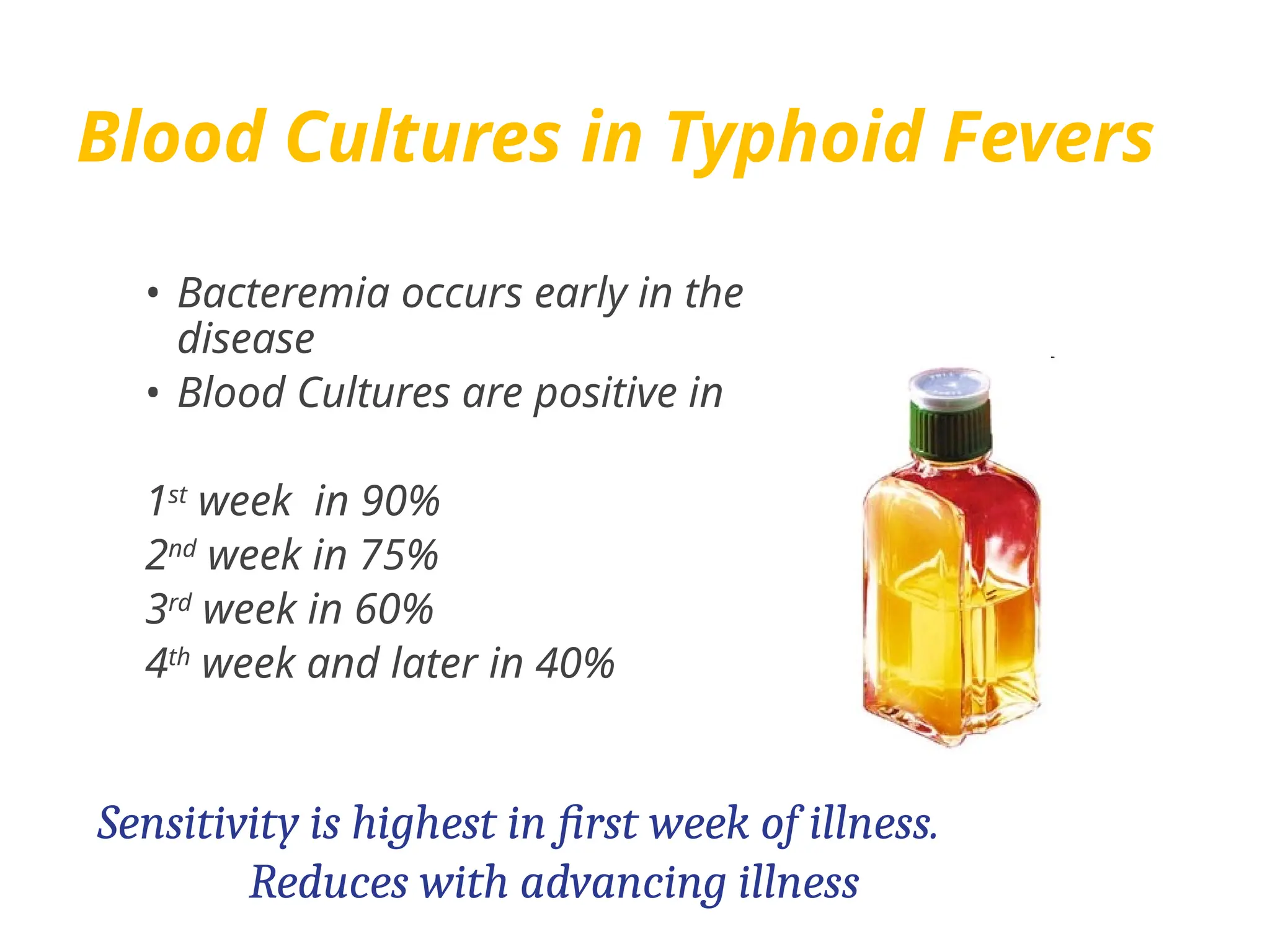
Blood Cultures inTyphoid Fevers
• Bacteremia occurs early in the
disease
• Blood Cultures are positive in
1st
week in 90%
2nd
week in 75%
3rd
week in 60%
4th
week and later in 40%
Sensitivity is highest in first week of illness.
Reduces with advancing illness
35.
• Amount ofblood - 5ml in children
10 ml in adults
Incubated at 37 degrees for 7 days
Interpretation-
If bottles show positive growth on 1,2,3 days then the bottles
should be cultured.
All the bottles should be subcultured on 7th
day before being
declared as negative.
36.
Bone marrow culture
•S.Typhi is an intracellular pathogen in
reticuloendothelial cells of body including
bonemarrow.
• Median Bacterial count-9CFU/ml
compared to blood 0.3 CFU/ml
(Bone marrow:peripheral blood ratio of
bacteremia-
4.8 in 1st
week 158 in 3rd
week
• Sensitivity -90%
• Advantages-good even in late disease despite
prior antibiotic therapy .
37.
Other methods inIsolation of Enteric
Pathogens
1st week B Blood cultre
(bone marrow culture
rarely)
2nd week A Agglutination test
3rd week S Stool culture
4th week U Urine cultre
SEROLOGICAL TESTS
• WIDALTEST
• Agglutins appear in blood by end of 1st week.
• O-agglutinins rises rapidly (4 fold in 10-14 days) ,
Persist for a month and disapear in a year.
• H-Agglutinins rises slows and persist for years.
• Hence O-agglutinin important in recent infection
And H-agglitinin indicate past infection or
immunisation.
40.
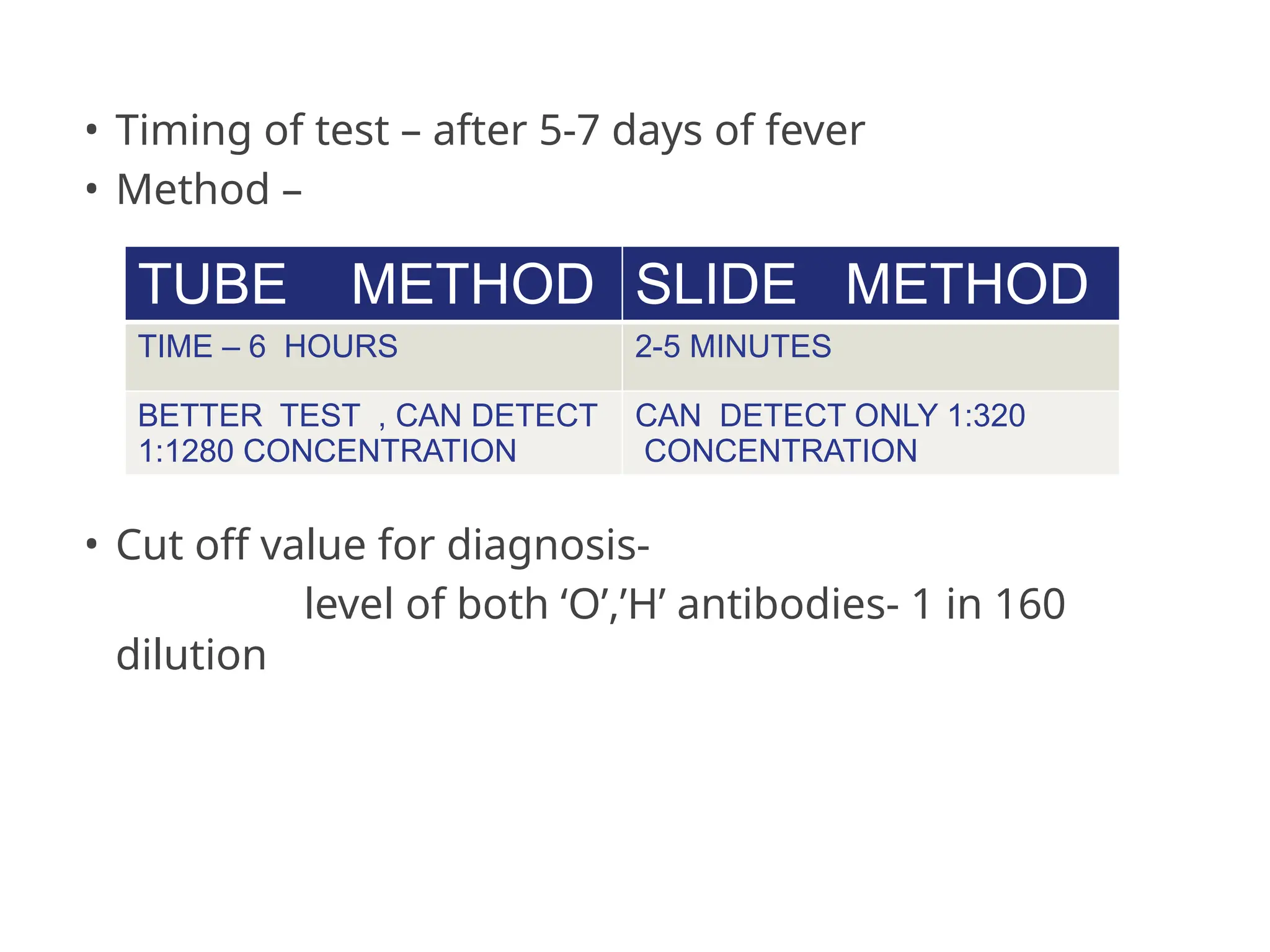
• Timing oftest – after 5-7 days of fever
• Method –
• Cut off value for diagnosis-
level of both ‘O’,’H’ antibodies- 1 in 160
dilution
TUBE METHOD SLIDE METHOD
TIME – 6 HOURS 2-5 MINUTES
BETTER TEST , CAN DETECT
1:1280 CONCENTRATION
CAN DETECT ONLY 1:320
CONCENTRATION
41.
• Demonstration ofa rise in titer of antibodies , by
testing paired blood samples 10-14 days apart is
preferred.
• Anamnestic response-
persons who have had prior infection or
immunization may develop an Anamnestic
response during an unrelated fever.
differentiated by repetition of test after 1 week
42.
1.Typhidot test: detectsIgM and IgG antibodies against the outer
membrane protein (OMP)
2.lDLTubex test: detects IgM O9 antibodies within few minutes.
3.lgM dip stick test and ELISA: detects anti-LPS IgM antibodies.
4.Dot blot assay: detects IgG antibodies.
5. Nested PCR analysis using H1-d primers.
New diagnostic tests
PREVENTION
• Enteric feveris a WASH disease
• Unsafe water sanitation and food with poor hygiene practices
51.
How can Typhoidbe avoided?
• Avoid risky foods or drinks
• Get vaccinated
• Use only clean water
• Ask for drinks without ice unless you know
where it’s coming from
• Only eat foods that have been thoroughly
cooked
• Avoid foods and drinks from street vendors
52.
CONTROL OF SANITATION
•PROTECTION AND PURIFICATION OF DRINKING WATER SUPPLY
• IMPROVEMENT OF BASIC SANITATION
• PROMOTION OF FOOD HYGIENE
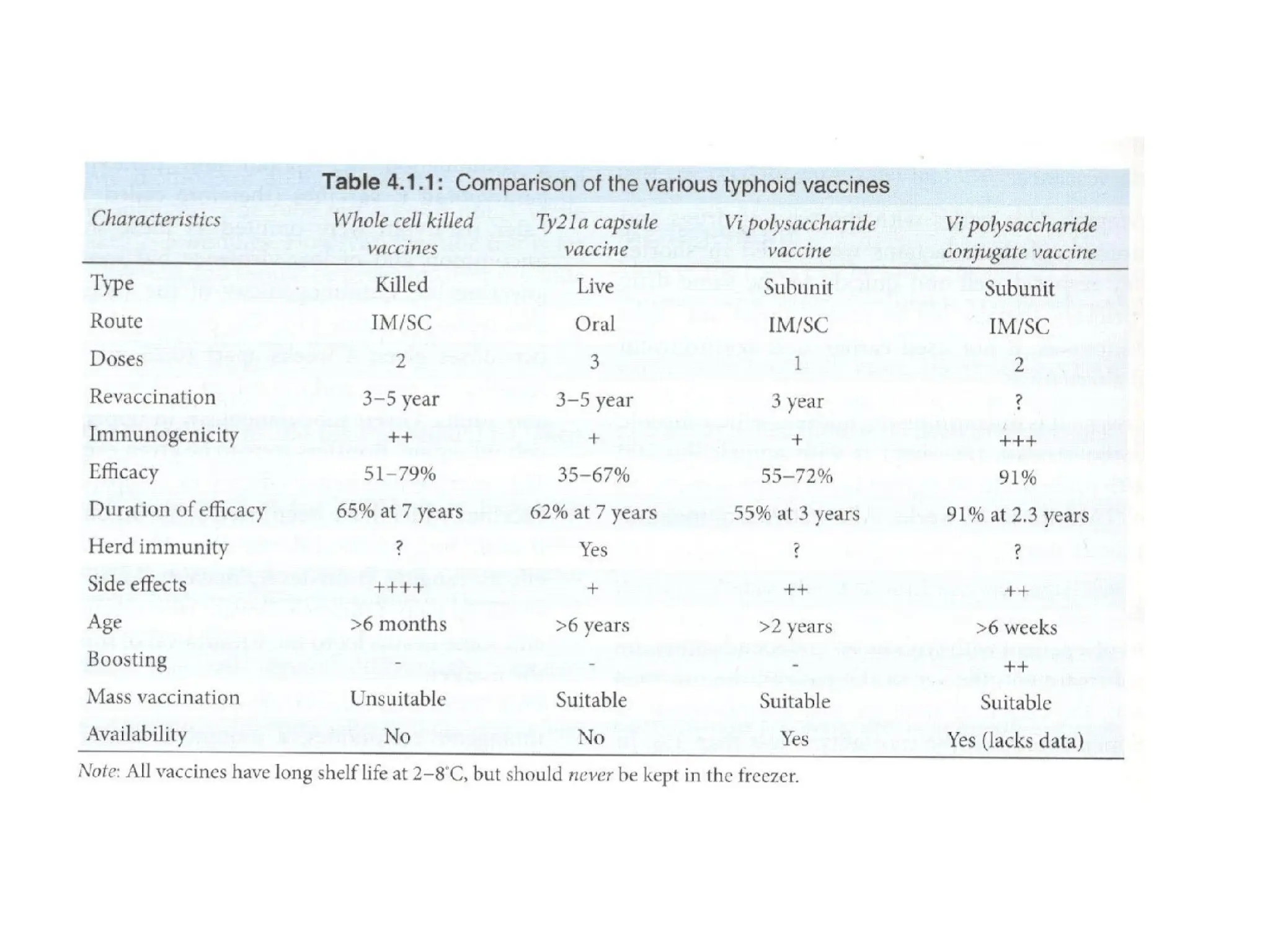
VACCINES
1. Classic heatinactivated whole cell vaccine
• Very high side effects
• Currently withdrawn
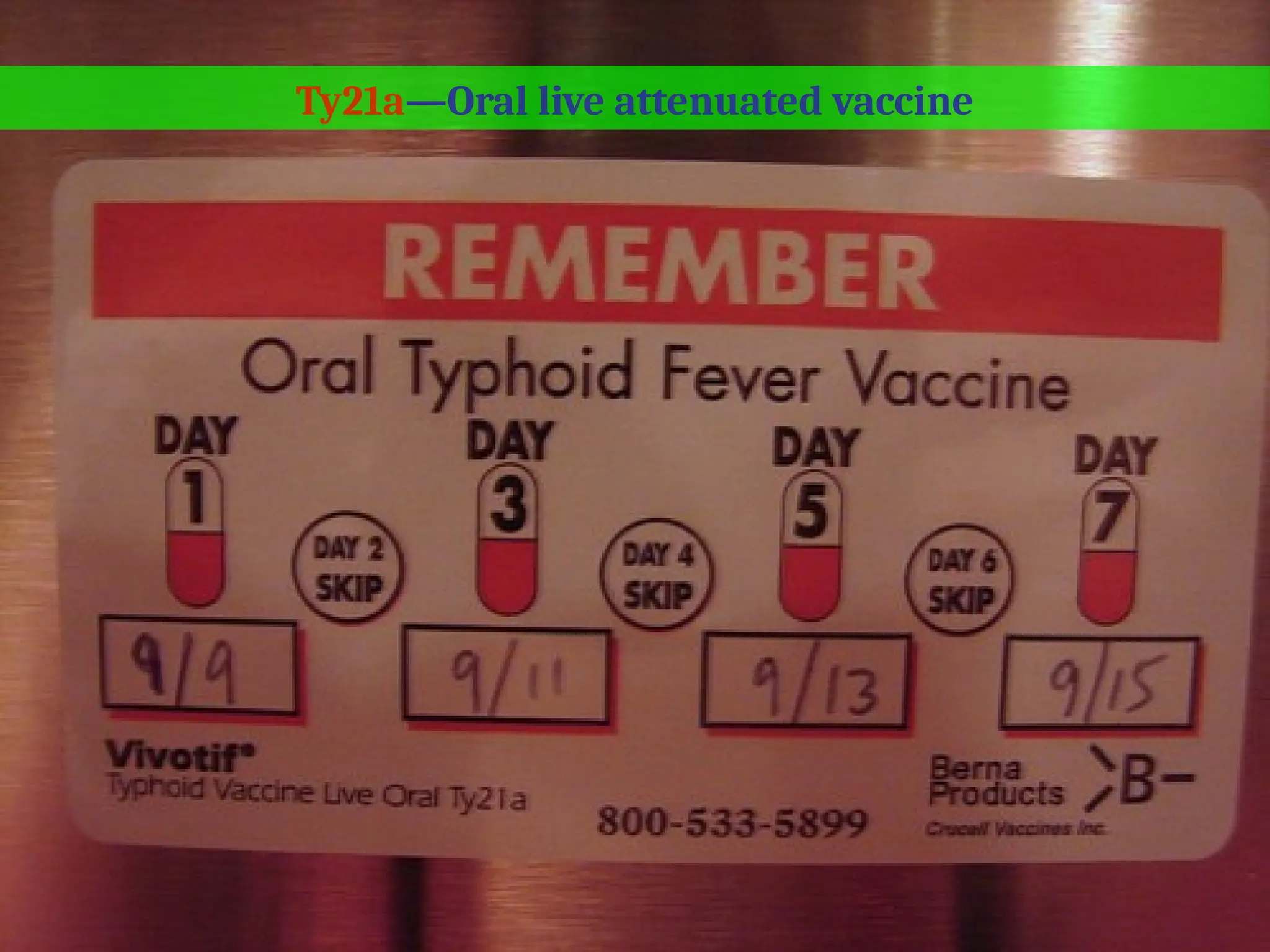
2. Ty21a ( oral live attenuated )
• Efficacy 67-82% for up to 5 years
• 3-4 doses
• Capsules
• Repeated every 3 years
• For children above 5 years
• Drugs to stop : Proguanil, mefloquine and
antibiotics 3 days before and 3 days after.
57.
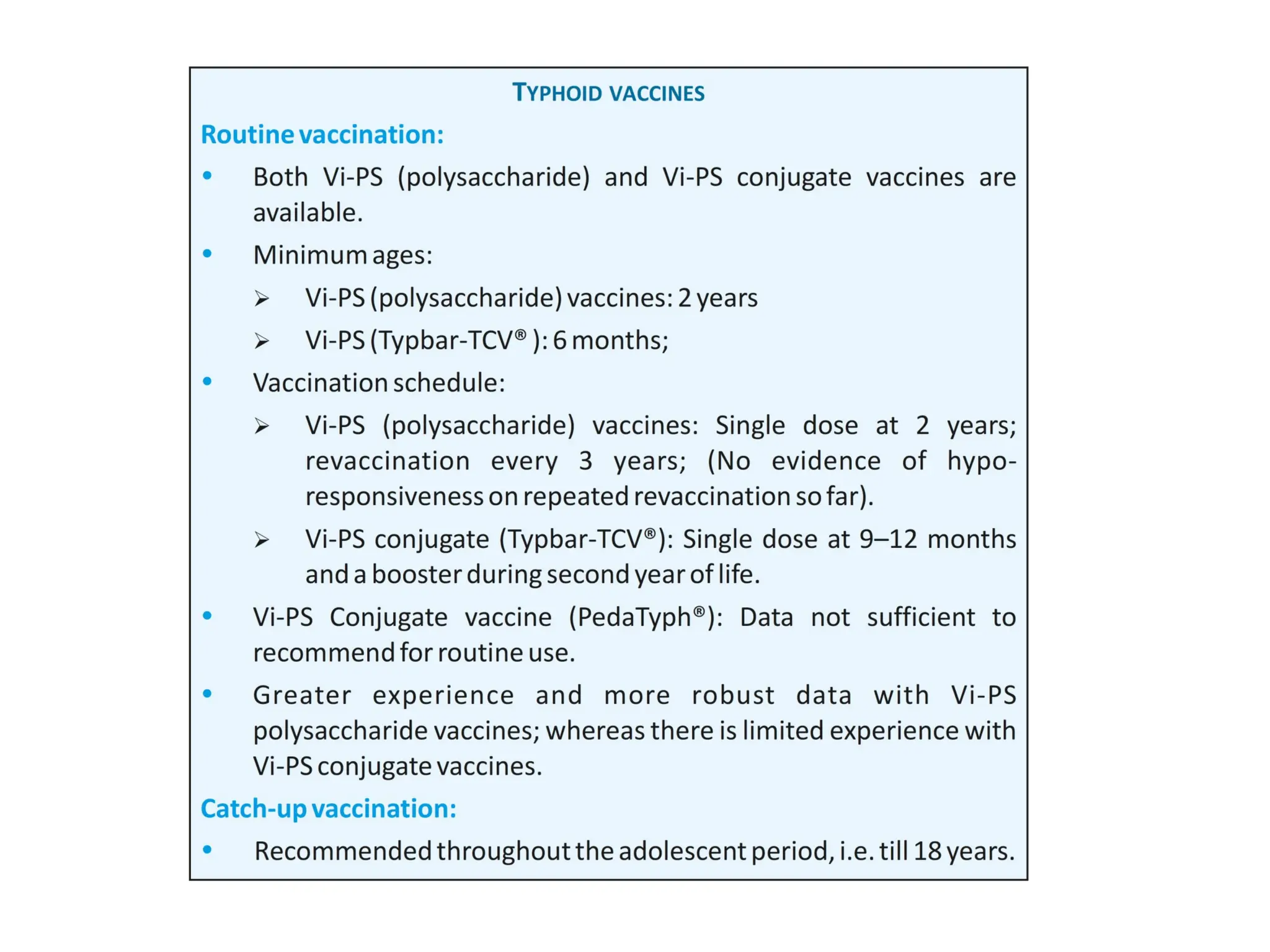
3. Vi capsularpolysaccharide
• Single intramuscular
• For more than equal to 2 years
• Efficacy 70-80%
• Repeat dose every 3 years
• Traveler's to endemic areas
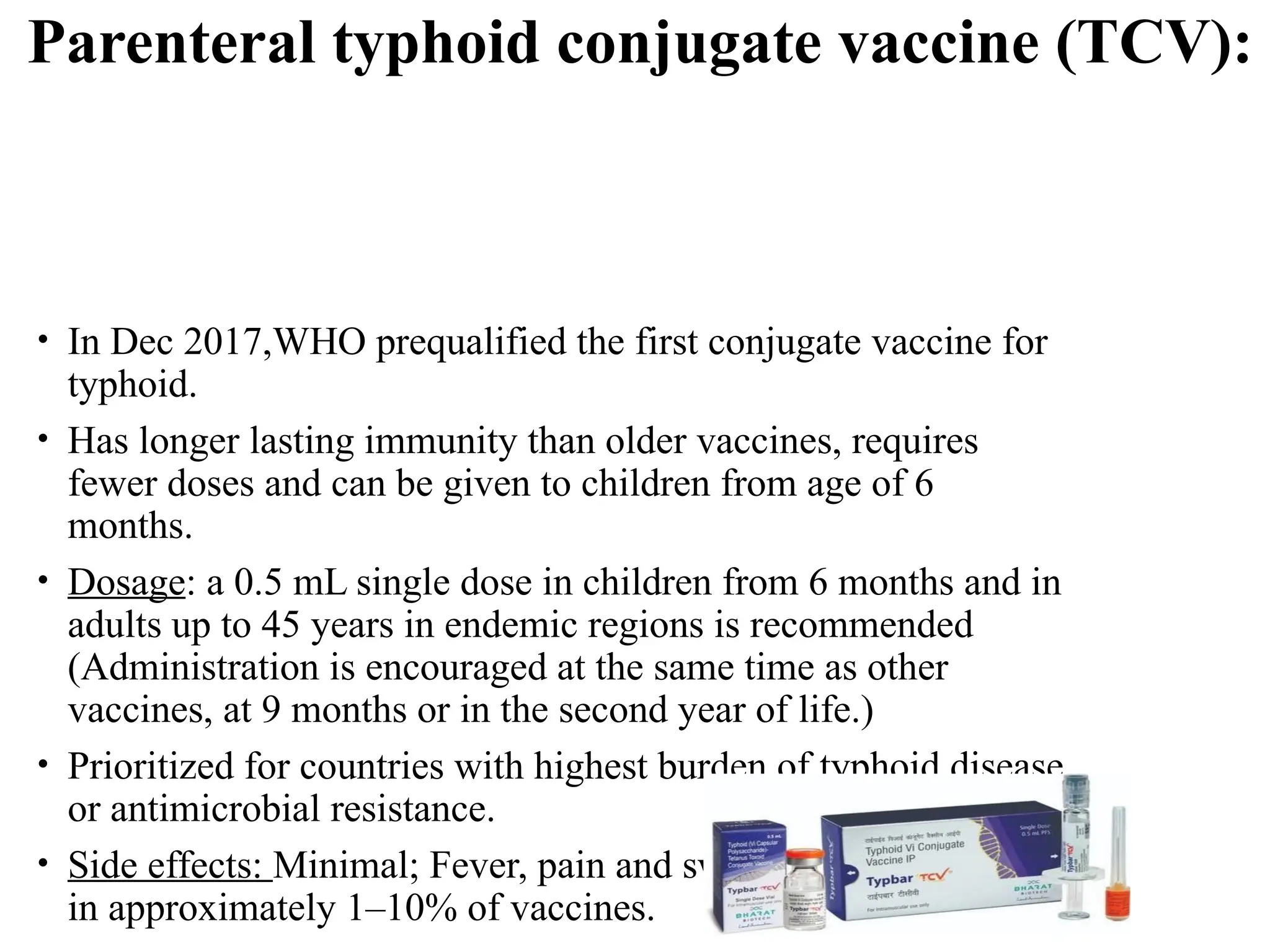
4. Protein conjugated Vi polysaccharide
• Very effective
• In Dec2017,WHO prequalified the first conjugate vaccine for
typhoid.
• Has longer lasting immunity than older vaccines, requires
fewer doses and can be given to children from age of 6
months.
• Dosage: a 0.5 mL single dose in children from 6 months and in
adults up to 45 years in endemic regions is recommended
(Administration is encouraged at the same time as other
vaccines, at 9 months or in the second year of life.)
• Prioritized for countries with highest burden of typhoid disease
or antimicrobial resistance.
• Side effects: Minimal; Fever, pain and swelling were reported
in approximately 1–10% of vaccines.
Parenteral typhoid conjugate vaccine (TCV):
Who should getthe Typhoid Vaccine?
• Travelers to parts of the
world where Typhoid
Fever is very common.
• People who work with
or come in contact with
a carrier of the disease.
• Laboratory analysts
who work with the
Salmonella Typhi
bacteria.
64.
Management of carriers
•An individual is considered to be a chronic carrier if he or she is
asymptomatic and continues to have positive stool or rectal swab
cultures for S. typhi a year following recovery from acute illness.
• The rate of carriage is slightly higher among female patients,
patients older than 50 years, and patients with cholelithiasis or
schistosomiasis.
• If cholelithiasis or schistosomiasis is present the patient probably
requires cholecystectomy or antiparasitic medication in addition
to antibiotics in order to achieve bacteriological cure
65.
• amoxicillin orampicillin (100 mg per kg per day)
plus
probenecid ( 23 mg per kg for children) or
• TMP-SMZ (160 to 800 mg twice daily)
• Given for 6 weeks
• 60% cure rate
66.
• 750 mgof ciprofloxacin or
400 mg of norfloxacin
• twice daily for 28 days
• 80 % cure rate
67.
• Carriers shouldbe excluded from any activities involving food
preparation and serving, as should convalescent patients and any
persons with possible symptoms of typhoid fever.
• Vi antibody determination has been used as a screening
technique to identify carriers among food handlers and in
outbreak investigations. Vi antibodies are very high in chronic S.
typhi carriers











































































![Circle of willis (finql)[1].pptx anatomy](https://cdn.slidesharecdn.com/ss_thumbnails/circleofwillisfinql1-250913015401-7ca582c5-thumbnail.jpg?width=640&height=640&fit=bounds)






















