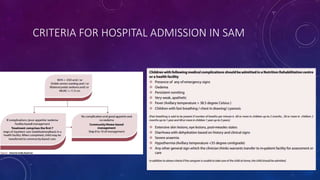
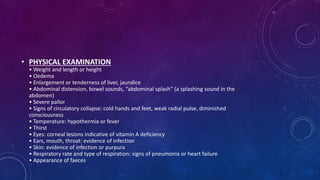
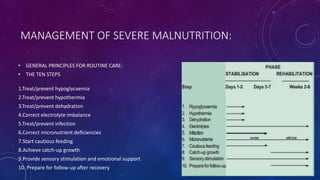
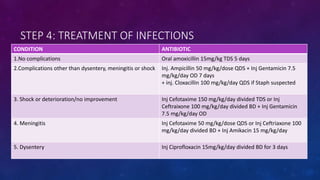
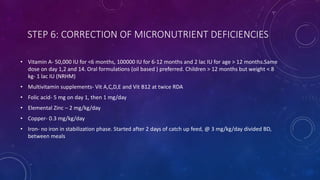
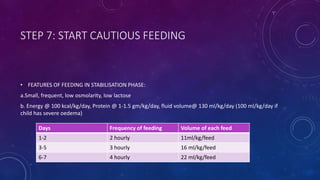
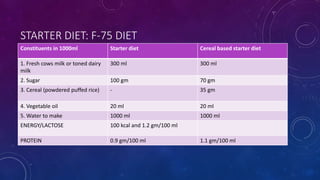
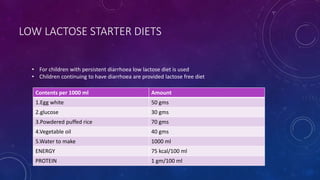
The document summarizes key information about severe acute malnutrition (SAM). It discusses the global burden of malnutrition, criteria for identifying SAM, pathophysiology, changes in body organs and metabolism, screening and outpatient/inpatient management. It provides details on the stabilization, transition and rehabilitation phases of hospital management, following the 10 steps for routine care which include treating hypoglycemia, hypothermia, dehydration and infections, and correcting electrolyte and micronutrient deficiencies. It also describes starter diets like F-75.