Downloaded 75 times







![Management Steps
Detailed History and Examination [SAMPLE]Step02
InvestigationsStep03
Empirical TreatmentStep 04
Supportive CareStep05
Rapid Assessment and Stabilization [ABCDE]Step01
Prevention/treatment of complications & rehabilitationStep06
Management Steps](https://image.slidesharecdn.com/encephelitisencephalopathies-200520045019/85/Encephalitis-Encephalopathies-13-320.jpg)

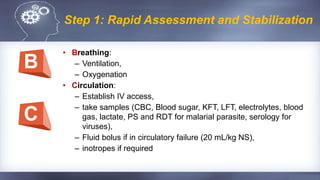






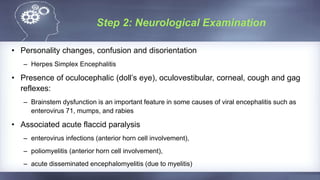





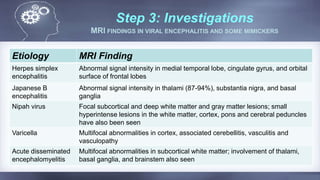




















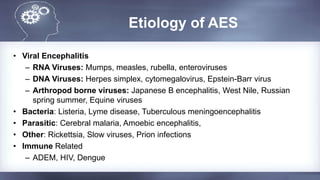
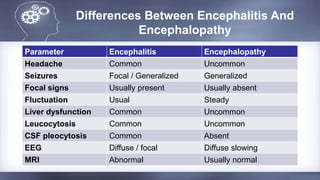
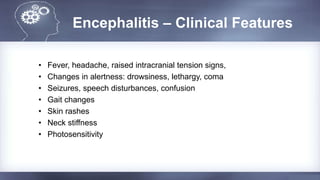
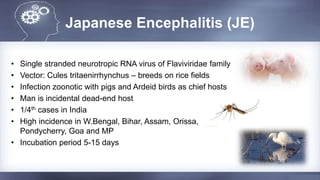
This document discusses encephalitis and encephalopathies in children. It begins with important definitions such as encephalopathy, acute encephalitis syndrome, encephalitis, and meningoencephalitis. It then discusses the types and etiologies of encephalitis including infectious causes such as viral, bacterial, parasitic and immune related causes as well as non-infectious causes. Specific conditions discussed in more detail include Japanese encephalitis, herpes simplex virus encephalitis, and metabolic encephalopathies. The document concludes with sections on the clinical features, investigations, management steps including empirical treatment and supportive care, and preventive strategies for encephalitis.























































































