Encephalitis is inflammation of the brain parenchyma that is usually caused by viral infection. Common viruses include herpes simplex virus type 1 and West Nile virus. Clinical features include altered mental status, seizures, and focal neurological deficits. Diagnosis involves CSF analysis showing pleocytosis and identifying the virus through PCR or serology. Treatment involves antivirals for suspected viruses and managing increased intracranial pressure and seizures. Prognosis depends on the specific virus and early initiation of treatment.
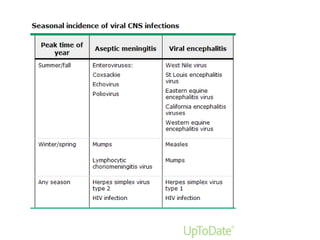


![Empiric therapy
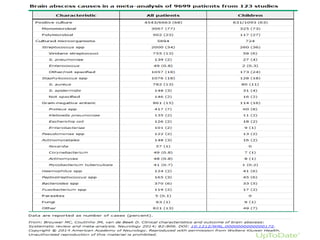
For patients with a brain abscess arising from
an oral, otogenic, or sinus source
Metronidazole (7.5 mg/kg [usually 500 mg]
every six to eight hours) PLUS either
ceftriaxone (2 g IV every 12 hours) or
cefotaxime (2 g IV every four to six hours).](https://image.slidesharecdn.com/encephelitisandbrainabcess-210911114205/85/Encephelitis-and-brain-abcess-58-320.jpg)
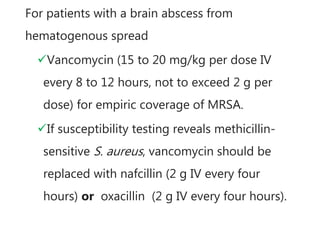
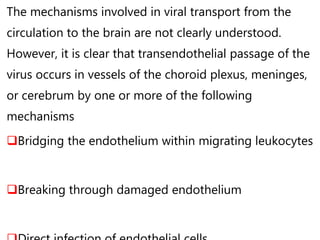
![For brain abscesses with an unknown source,
we recommend treatment with:
Vancomycin (15 to 20 mg/kg per dose IV every 8 to 12 hours,
not to exceed 2 g per dose) PLUS Metronidazole (7.5 mg/kg
[usually 500 mg] IV every six to eight hours) PLUS Ceftriaxone
(2 g IV every 12 hours) or cefotaxime (2 g IV every four to six
hours). Cefepime (2 g IV every eight hours) should be used
instead of ceftriaxone or cefotaxime if Pseudomonas is
possible.](https://image.slidesharecdn.com/encephelitisandbrainabcess-210911114205/85/Encephelitis-and-brain-abcess-61-320.jpg)