Downloaded 700 times




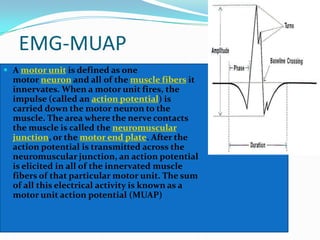



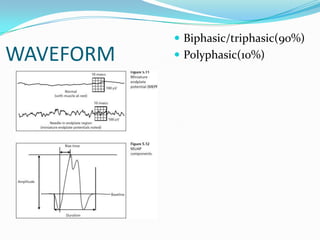





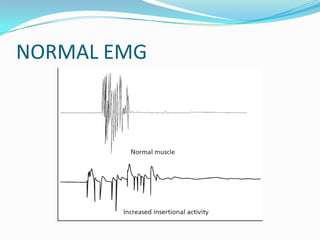

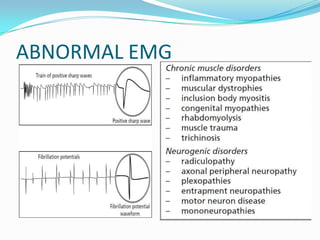

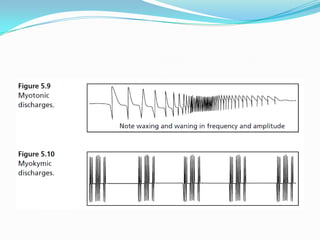






This document discusses electrodiagnostic tests used to evaluate neuromuscular disorders, including nerve conduction studies and electromyography (EMG). It provides details on reaction of regeneration testing, strength-duration curves, chronaxie and rheobase measurements, galvanic twitch-tetanus ratios, nerve excitability testing, EMG motor unit action potentials, common mode rejection ratios, waveform types, EMG circuitry, electrode types, normal and abnormal EMG findings, indications for EMG testing, and findings that can be observed on EMG that provide information about muscle and nerve diseases.











































































































