Downloaded 1,115 times





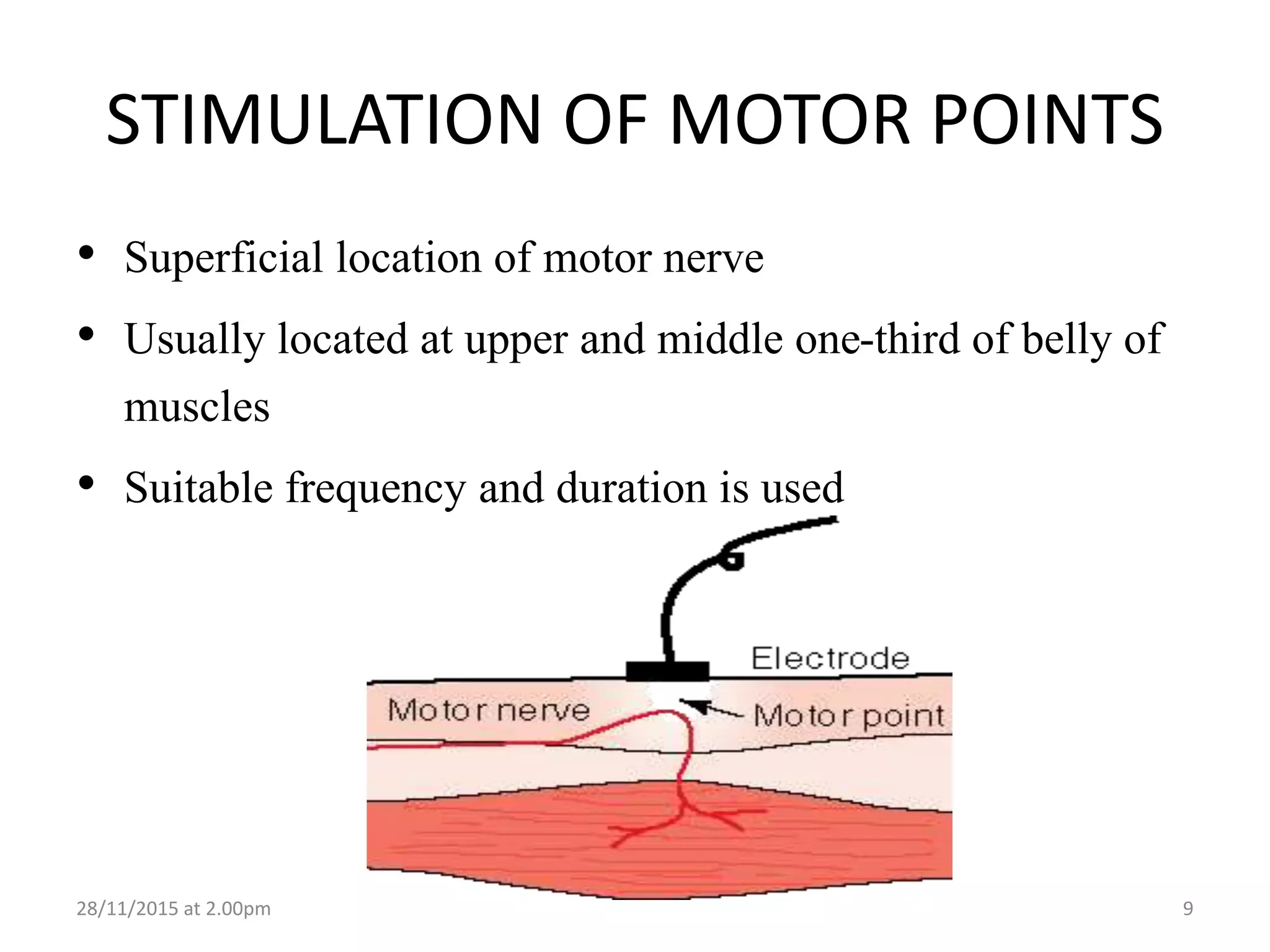




























Electrical stimulation involves applying modified electric currents to excitable tissues like nerves and muscles to produce therapeutic benefits. Direct and alternating currents can be used to stimulate tissues. Faradic and interrupted galvanic currents of varying durations and frequencies are used for stimulation of normal and denervated muscles. Electrical stimulation modalities like TENS, NMES, FES and interferential therapy are used for pain management and rehabilitation by stimulating nerves and muscles. Precise electrode placement is important for effective stimulation.



































































