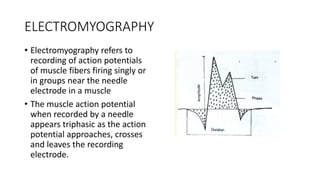
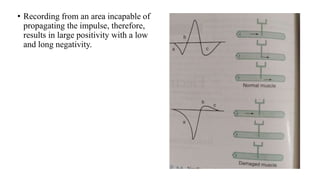
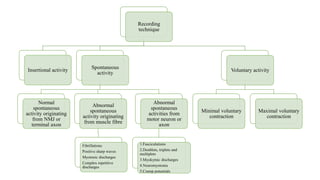
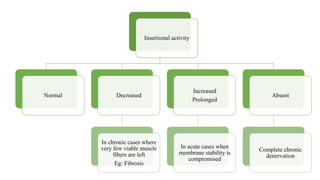
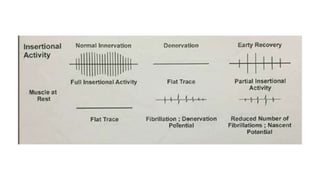
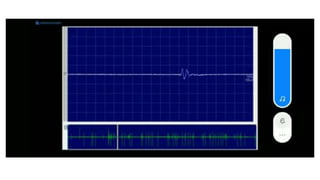
This document provides information about electromyography (EMG). EMG is a test that evaluates the health and function of muscles and the nerve cells that control them. It involves inserting a needle electrode into a muscle to record electrical activity from muscle fibers and nerves. Abnormal spontaneous electrical activities in muscles can indicate neurological or muscular disorders. EMG is useful for diagnosing conditions like amyotrophic lateral sclerosis, myasthenia gravis, and muscular dystrophy. It provides information about the location and severity of nerve or muscle damage.



































![ELECTRO MYO GRAM [EMG]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/electromyogramemg-1-230303140416-5e58de8a-thumbnail.jpg?width=640&height=640&fit=bounds)




































