Ectopic pregnancy
•
18 likes•7,765 views

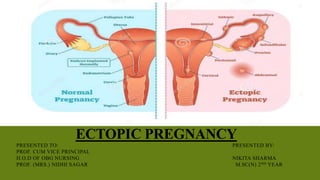
Ectopic pregnancy occurs when a fertilized egg implants outside of the uterus, usually in the fallopian tubes. There are several types of ectopic pregnancies classified by location, with tubal pregnancies making up about 90% of cases. Risk factors include previous ectopic pregnancy, PID, tubal ligation or surgery. Symptoms include abdominal pain and vaginal bleeding. Diagnosis involves ultrasound, serum hCG levels, and sometimes laparoscopy. Treatment options range from expectant management for very early, low risk cases to surgical intervention like salpingectomy for ruptured ectopic pregnancies.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ectopic pregnancy
Similar to Ectopic pregnancy (20)
More from Nikita Sharma
More from Nikita Sharma (20)
Recently uploaded
Recently uploaded (20)
Ectopic pregnancy
- 1. ECTOPIC PREGNANCY PRESENTED TO: PRESENTED BY: PROF. CUM VICE PRINCIPAL H.O.D OF OBG NURSING NIKITA SHARMA PROF. (MRS.) NIDHI SAGAR M.SC(N) 2ND YEAR
- 6. CLASSIFICATION NON TUBAL ECTOPIC PREGNANCY (2-5% RARE) OVARIES BROAD LIGAMENTS CERVIX ABDOMINAL CAVITY & PERITONEUM
- 7. HETEROTOPIC PREGNANCY When pregnancy occur in both the womb and the tube at the same time.
- 8. ETIOLOGY/ RISK FACTORS HISTORY OF PID PREVIOUS ECTOPIC PREGNANCY HISTORY OF TUBAL LIGATION TUBAL RECONSTRUCTIVE SURGERY CONTRACEPTIVE FAILURE
- 9. ETIOLOGY/RISK FACTORS ART WHEN TUBES ARE DAMAGED IUD USE PREVIOUS INDUCED ABORTION TUBAL ENDOMETRIOSIS HISTORY OF INFERTILITY
- 10. OTHER RISK FACTORS Age 35-45 yrs Previous induced abortion Previous pelvic surgeries Cigarette smoking DES Exposure in Utero Infertility Salpingitis Isthmica Nodosa Genital Tuberculosis Fundal Fibroid & Adenomyosis of tube Transperitoneal migration of ovum
- 11. Iffy hypothesis – “Theory of reflux” menstural fluid throw the fertilised ovum into the tube Factors facilitating nidation of ovum in tube: - Premature degeneration of zona pellucida - Increased decidual reaction - Tubal endometriosis
- 12. EVOLUTION Tubal pregnancies rapidly invade the mucosa, feeding from the tubal vessels, which become enlarged and engorged. The segment of the affected tube is distended as the pregnancy grows. Possible outcomes of such abnormal gestations are as follows:
- 13. MORBIDANATOMY Changes Implantation- intercolumnar or between mucosal flods Decidual change minimal Muscle hyperplasia & Hypertrophy min. Intramuscular implatation Pseudocapsule formation Trophoblast invasion-erosion of blood vessel The pregnancy is unable to survive owing to its poor blood supply, thus resulting in a tubal abortion and resorption, (rare) Tubal Rupture Isthmic – 6-8 wks, Ampullary – 8-12wks, Interstitial -4 months Abortion is common in ampullary pregnancies,whereas rupture is in isthmic.
- 14. ARIAS – STELLA REACTION Arias – Stella reaction is charecterised by a benign, focal and unusual decidual changes in the presence of chorionic tissue, Loss of polarity Pleomorphism Hyperchromatic nuclei Vacuolated cytoplasm Intraluminal budding Though seen in Ectopic Pregnancy but is not specific for it and can also be seen in uterine pregnancy. • It occurs due to the effect of progesterone.
- 16. TUBAL PREGNANCY
- 17. PATHOPHYSIOLOGY The trophoblast develops in the fertilized ovum and invades deeply into the tubal wall. Following implantation, the trophoblast produces hCG which maintains the corpus luteum. The corpus luteum produces oestrogen and progesteronewhich change the secretory endometrium into decidua. The uterus enlarges up to 8 weeks and becomes soft. The tubal pregnancy does not usually proceed beyond 8-10weeksdue to: > lack of decidual reaction in the tube, > the thin wall of the tube, > the inadequacy of tubal lumen, > bleeding in the site of implantation as trophoblast invades.
- 18. PATHOPHYSIOLOGY Separation of the gestational sac from the tubal wall leads to its degeneration, and fall of hCG level, regression of the corpus luteum and subsequent drop in the oestrogen and progesteronelevel. This leads to separation of the uterine decidua with uterine bleeding Fate of tubal pregnancy Tubal mole Tubal abortion Tubal rupture
- 20. FATE OF TUBAL PREGNANCY 1 Tubal mole: The gestational sac is surrounded by a blood clot and retained in the tube. This may remain for long period in the tube and forms so called (chronic ectopic pregnancy),or they may be gradually absorbed (involution) 2 Tubal abortion: This occurs more if ovum had been implanted in the ampullary portion of the tube. Separation of the gestational sac is followed by its expulsion into the peritoneal cavity through the tubal ostium. Rarely, reimplantation of the conceptus occurs in another abdominal structure leads to secondary abdominal pregnancy.
- 21. Fate of tubal pregnancy If expulsion was complete the bleeding usually ceases but it may continue due to incomplete separation or bleeding from the implantation site.
- 22. FATE OF TUBAL PREGNANCY 3-Tubal rupture: More common if implantation occurs in the narrower portion of the tube which is the isthmus. Rupture may occur in the anti-mesenteric border of the tube. Usually profuse bleeding occurs → intraperitoneal haemorrhage. If rupture occurs in the mesenteric border of the tube, broad ligament haematoma will occur.
- 23. PRESENTATION Early symptoms are either absent or subtle. Clinical presentation of ectopic pregnancy occurs at a mean of 7.2 weeks after the last normal menstrual period, with a range of 5 to 8 weeks The most common presenting symptoms that are suggestive for EP are:
- 24. CLINICAL TRAID (3AS) Amenorhea Ectopic pregnancy Abdominal pain Abnormal vaginal bleeding
- 25. SYMPTOMS Pain and discomfort • In the Lower back , abdomin, or pelvis. Usually unilateral • Pain may be confused with a strong stomach pain, it may also feel like a strong cramp • Shoulder pain. This is caused by free blood tracking up the abdominal cavity and irritating the diaphragm, and is an ominous sign. • Pain while urinating • Pain while having a bowel movement
- 26. SYMPTOMS Bleeding • Vaginal (external)bleeding usually mild. An ectopic pregnancy is usually a failing pregnancy and falling levels of progesterone from the corpus luteum on the ovary cause withdrawal bleeding. • Internal bleeding (hematoperitoneum) is due to hemorrhage from the affected tube. • Dizziness, headache, weakness, fainting all may happen due to bleeding.
- 27. SIGNS General examination: • signs of early pregnancy (Breast tenderness, nausea and vomitig, change of appetite …) • Weakness, pallor, hypotension and tachycardia, tachypnea due to bleeding. Abdominal examination: most constant feature. It is acute, agonizing or colicky. Pain is located at lower abdomen: unilateral, bilateral or may be generalized. Shoulder tip pain (25%) – referred pain due to diaphragmatic irritation from haemoperitoneum may be present ( DANFORTH’S SIGN)
- 28. SIGNS Vaginal examination: • Vaginal spotting • Bluish vagina and bluish soft cervix. • Uterus is slightly enlarged and soft. • Marked pain in one iliac fossa on moving the cervix from side to side. • Ill defined tender mass may be detected in one adnexa in which arterial pulsation may be felt. • Speculum or bimanual examination should not be performed unless facilities for resuscitation are available, as this may induce rupture of the tube
- 29. UNRUPTURED ECTOPIC High degree of suspicion & ectopic conscious clinician can diagnose. Diagnosed accidentally in Laparoscopy or Laparotomy C/F – delayed period, spotting with discomfort in lower abdomen. P/A – tenderness in lower abdomen P/V should be done gently uterus is normal size, firm small tender mass may be felt in the fornix Investigations- TVS, radioimmunoassay of β-HCG and Laparoscopy
- 30. DIAGNOSIS Patient with acute ectopic can be diagnosed clinically. Blood should be drawn for Hb%, CBC, blood grouping and cross matching,.Serology and Coagulation profile. Should be catheterized to know urine output. Bed side test:- 1. Urine pregnancy test:- positive in 95% cases. ELISA is sensitive to 10-50 mlU/ml of β hCG and can be detected on 24th day after LMP. 2. Culdocentesis:- (70-90%) Can be done with 16-18 G lumbar puncture needle through posterior fornix . Positive tap is 0.5ml of non clotting blood.
- 31. DIAGNOSIS ▪ Imaging:- 1. Ultra Sonography- a) Transvaginal Sonography (TVS): Is more sensitive It detect intrauterine gestational sac at 4-5wks and at S-β hCG level as low as 1500 IU/L .
- 32. ENDOMETRIAL CAVITY -A trilaminar endometial pattern seen -pseudogestational sac -decidual cyst may be seen PSEUDOSAC – All pregnancies induce an endometrial decidual reaction, and sloughing of the decidua can create an intracavitary fluid collection called a pseudosac Early Gestational Sac Pseudosac Location Eccentrically located Midline within E.cavity Shape Round-shape Irregular Border Double Ring sign Vascularity High Avascular Pattern Peripheral -
- 33. b) Color Doppler Sonography(TV-CDS): - Improve the accuracy. - Identify the placental shape (ring-of-fire pattern) and blood flow outside the uterine cavity. c) Transabdominal Sonography: - can identify gestational sac at 5-6 wks - S-β hCG level at which intrauterine gestational sac is seen by TAS is 1800 IU/L.
- 34. USG PICTURE 1.‘Bagel’ sign – Hyperechoic ring around gestational sac in adnexal region 2. ‘Blob’ sign – Seen as small inconglomerate mass next to ovary with no evidence of sac or embryo. 3. Adnexal sac with fetal pole and cardiac activity is most specific. 4. Corpus luteum is useful guide when looking for EP as present in 85% cases in Ipsilateral ovary.
- 35. Hyperechoic ring around gestational sac in adnexal region
- 36. Ring sign — a hyperechoic ring around an extrauterine gestational sac.
- 37. 2. β-HCG Assay- a) Single β-HCG: little value b)Serial β-HCG: is required when result of initial USG is confusing. - When hCG level < 2000 IU/L doubling time help to predict viable Vs nonviable pregnancy. -Rise of β-HCG <66% in 48 hrs indicate ectopic pregnancy or nonviable intrauterine pregnancy . Biochemical pregnancy is applied to those women who have two β-HCG values >10 IU/L
- 38. 3. SERUM PROGESTERONE – level >25 ngm/ml is suggestive of normal intrauterine pregnancy. level <15 ngm/ml is suggestive of ectopic pregnancy. level <5 ngm/ml indicates nonviable pregnancy, irrespective of its location. 4. Diagnostic Laparoscopy (Gold standard)– Can be done only when patient is haemodynamically stable. -It confirms the diagnosis and removal of ectopic mass can be done at the same time.
- 39. DIAGNOSIS 5. Dilatation & Curettage – Is recommended in suspected case of incomplete abortion vs ectopic pregnancy. Identification of decidua without chorionic villi is suggestive of extra uterine pregnancy. “Arias-Stella” endometrial reaction is suggestive but not diagnostic of ectopic pregnancy.
- 40. SUSPECTED ECTOPIC PREGNANCY Urine Pregnancy test positive Transvaginal USG IU sac No IU sac Quantitative S-hCG + S progesterone < 66% rise in 48 hr or S progesterone < 5-10 ng/ml D & C Villi present Incomplete abortion Villi absent Laparoscopy >66% rise in 48 hr or S progesterone > 5-10 ng/ml Repeat S-hCG in 48 hrs till USG discrimination zone No sac IU sac Continue to monitor
- 41. DIFFERENTIAL DIAGNOSIS Acute Ectopic 1. Rupture corpus luteum of pregnancy 2. Rupture of chocolate cyst 3. Twisted ovarian cyst 4. Torsion / degeneration of pedunculated fibroid 5. Incomplete abortion 6. Acute Appendicitis 7. Perforated peptic ulcer 8. Renal colic 9. Splenic rupture
- 42. MANAGEMENT Expectant management Medical management Surgical management SystemicLocal (USG or Laparoscopic) salpingocentesis - Methotrexate - Potassium chloride - Prostagladin(PGF2α) - Hypersmolar glucose - Actinomycin D - Mifepristone Methotrexate Radical Salpingectomy Conservative -Salpingostomy -Salpingotomy - Segmental resection -Milking or fimbria expression
- 43. MANAGEMENT OF ECTOPIC- PRINCIPLE: Resuscitation and Laparotomy/Laparoscopy ANTI SHOCK TREATEMENT: - IV line made patent, crystalloid is started - Blood sample for Hb, blood grouping & cross matching, BT - Folley’s catheterization done - Colloids for volume replacement LAPAROTOMY: Principle is ‘Quick in and Quick out’ - Rapid exploration of abdominal cavity is done - Salpingectomy is the definitive surgery (sent for HP study) - Blood transfusion to be given - Autotransfusion only when donated blood not available.
- 44. MANAGEMENT OF ECTOPIC PREGNANCY- Laparoscopy Preferred method if haemodynamically stable Tubal Patency no significant difference Followed by similar number of uterine pregnancy Shorter operative time Salpingostomy Less than 2cm size 10-15mm incision
- 46. MANAGEMENT OF UNRUPTURED ECTOPIC PREGNANCY OPTIONS: - SURGICAL- SURGICALLY ADMINISTERED MEDICAL(SAM) TREATMENT MEDICAL TREATMENT EXPECTANT MANAGEMENT
- 47. EXPECTANT MANAGEMENT IDENTIFICATION CRITERIA - : 1. Tubal ectopic pregnancies only 2. Haemodynamically stable 3. No rupture or bleeding 4. Adnexal mass of < 3.5 cm without heart beat. 5. Initial β HCG <1000 IU/L and falling in titre (single best) SUCCESS RATE - Upto 60% PROTOCOL: - Hospitalization with strict monitoring of clinical symptom - Daily Hb estimation - Serum β HCG monitoring 3-4 days until it is <10 IU/L - TVS to be done twice a week.
- 48. EXPECTANT MANAGEMENT Spontaneous resolution occurs in 72%,while 28% will need laparoscopic salpingostomy In spontaneous resolution, it may take 4-67 days (mean 20 days) for the serum HCG to return to non pregnant level. The percentage fall in serum HCG by day 7 is a better indicator than the percentage fall by day 2. Warning: - Tubal pregnancies have been known to rupture even when Serum HCG levels are low.
- 49. MEDICAL MANAGEMENT Surgery is the mainstay of T/t worldwide Medical M/m may be tried in selected cases CANDIDATES FOR METHOTREXATE (MTX) Unruptured sac < 3.5cm without cardiac activity S-hCG < 10,000 IU/L Persistant Ectopic after conservative surgery PHYSICIAN CHECK LIST CBC, LFT, RFT, S-hCG Transvaginal USG within 48 hrs Obtain informed consent Anti-D Ig if pt is Rh negative
- 50. MEDICAL MANAGEMENT METHOTREXATE: It can be used as oral,intramuscular ,intravenous usually along with folinic acid. Resolution of tubal pregnancy by systemic administration of Methotrexate was first described by Tanaka et al (1982) Mostly used for early resolution of placental tissue in abdominal pregnancy.Can also be used for tubal pregnancy. Mechanism of action-Methotrexate is a folic acid antagonist that inactivates the enzyme dihydrofolate reductase.Interferes with the DNA synthesis by inhibiting the synthesis of pyrimidines leading to trophoblastic cell death. Auto enzymes and maternal tissues then absorb the trophoblast.
- 51. MEDICAL MANAGEMENT Single dose Mtx 50mg/m² IM βHCG levels at days 4 & 7 •If difference ≥15% repeat weekly till ≤5IU/ml •If difference ˂15% between day 4 & 7 repeat dose & begin D₁ •If fetal Cardiac +ve at D₇ repeat D₁ Mtx •Surgical management if βHCG not ↓ or fetal cardiac +ve after 3 doses Two dose on Day 0, 4 Follow-up same as One dose regimen Variable doses 1. Mtx 1gm/kg IM D₁₃₅₇ 2. Leucovorin 0.1mg/kg IM D₂₄₆₈ Measure βHCG levels at D₁₃₅₇ . Continue alternate day regimen until βHCG levels decrease ≥15% in 48hrs, or 4 doses of Mtx given. Then, weekly βHCG levels until <5iu/ml
- 52. CONTD…… Advantages – Minimal Hospitalisation.Usually outdoor treatment Quick recovery 90% success if cases are properly selected Disadvantages- Side effects like GI & Skin Monitoring is essential- Total blood count, LFT & Serum HCG once weekly till it becomes negative
- 53. SURGICALLYADMINISTERED MEDICALTT (SAM) Aim- trophoblastic destruction without systemic side effects Technique- Injection of trophotoxic substance into the ectopic pregnancy sac or into the affected tube by- Laparoscopy or Ultrasonographically guided Transabdominal (Porreco, 1992) Transvaginal (Feichtingar, 1987) With Falloposcopic control (Kiss, 1993)
- 54. SURGICALLY ADMINISTERED MEDICAL Tt (SAM) Trophotoxic substances used- Methtrexate (Pansky, 1989) Potassium Chloride (Robertson, 1987) Mifiprostone (RU 486) PGF2 (Limblom, 1987) Hyper osmolar glucose solution Actinomycin D Advantage of local MTX : - Increase tissue concentration at local site - Decrease systemic side effects - Decrease hospitalization - Greater preservation of fertility Follow up: - Serum β HCG twice weekly till < 5 IU/L - TVS weekly for 4-6 weeks - HCG after 6 months for tubal patency
- 55. INSTRUCTION TO THE PATIENTS If T/t on outpatient basis rapid transportation should be available Refrain from alcohol, sunlight, multivitamins with folic acid, and sexual intercourse until S-hCG is negative. Report immediately when vaginal bleeding, abdominal pain, dizziness, syncope (mild pain is common called separation pain or resolution pain) Failure of medical therapy require retreatment Chance of tubal rupture in 5-10 % require emergency Laparotomy.
- 56. ECTOPIC CONSERVATIVE SURGERY Can be done Laparoscopically or by microsurgical laparotomy INDICATION: - Patient desires future fertility - Contralateral tube is damaged or surgically removed previously CHOICE OF TECHNIQUE: depends on - Location and size of gestational sac - Condition of tubes - Accessibility
- 57. VARIOUS CONSERVATIVE SURGERIES 1.Linear Salpingostomy: - Indicated in unruptured ectopic <2cm in ampullary region. - Linear incision given on antimesentric border over the site and product removed by fingers, scalpel handle or gentle suction and irrigation. - Incision line kept open (heals by secondary intention) 2. Linear Salpingotomy : - Incision line is closed in two layers with 7-0 interrupted vicryl sutures. 3. Segmental Resection & Anastomosis: - Indicated in unruptured isthmic pregnancy - End to end anastomosis is done immediately or at later date
- 58. 4. Milking or fimbrial Expression: - This is ideal in distal ampullary or infundibular pregnancy. - It has got increased risk of persistent ectopic pregnancy. ADVANTAGES OF LAPAROSCOPY - It helps in diagnosis, evaluation, and treatment . - Diagnose other causes of infertility. - Decreased hospitalization, operative time, recovery period, analgesic requirement. Follow up after conservative surgery - With weekly Serum β HCG titre till it is negative. - If titre increases methotrexate can be given.
- 59. CE 1.Gynecology & obstetrci by Ten teachers 19th edition 2.RCOG guidelines (Royal college of obstetric & gynecology) 3.ACOG(American college of obstetric & gynecology) 4.ASRM(American society of reproductive medicine) 5.Wikipedia .com 6.Livemedicine.co m
- 60. THANK YOU