
Downloaded 92 times















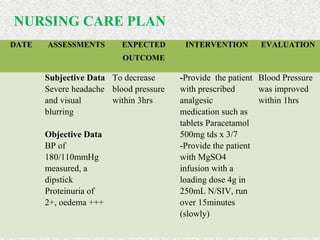

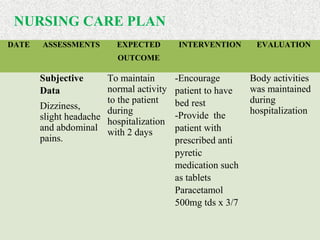









A 27-year-old woman was admitted to the hospital with severe pre-eclampsia at 35 weeks and 3 days of gestation. She had a blood pressure of 180/110 mmHg, proteinuria, edema, headache, and blurred vision. She received magnesium sulfate and antihypertensive medications. She later had a cesarean section under general anesthesia and delivered twins weighing 1.8 kg and 1.6 kg. The nursing care focused on monitoring her vital signs and symptoms, managing her blood pressure and fluids, providing rest and medications, and health education. Recommendations included improving equipment, guidelines, and staff training for managing severe pre-eclampsia.






















































![9_hypertension_(1)_(3)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/9hypertension131-230607084247-9b815ae1-thumbnail.jpg?width=640&height=640&fit=bounds)






































