This document discusses various topics related to abortion including definitions, incidence rates, classifications, etiology, clinical features, management, and complications. Some key points:
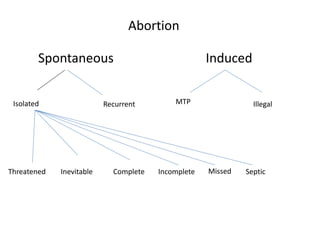
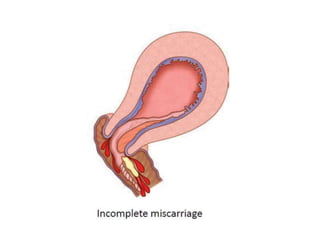
- Abortion is defined as the expulsion of an embryo or fetus weighing less than 500g. Common classifications include threatened, inevitable, incomplete, complete, missed, and septic abortion.
- Incidence rates are 10-20% of clinical pregnancies, with 75% occurring before 16 weeks. Rates vary by maternal age and history of miscarriage.
- Etiology can include fetal factors like genetic abnormalities and maternal factors like endocrine/metabolic issues, infections, immunological disorders, and environmental exposures.
- Clinical features

![Complications
• Retaining the products for long time can lead
to sepsis
• DIC [Disseminated Intravascular Coagulation]
– (very rare) in gestations exceeding 16 weeks](https://image.slidesharecdn.com/abortion-151022113610-lva1-app6891/85/Abortion-27-320.jpg)



































![ABORTION -POST ABORTIVE CARE[1][2] ner.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abortion-postabortivecare12ner-250903092827-23f6f291-thumbnail.jpg?width=640&height=640&fit=bounds)
































