Downloaded 58 times











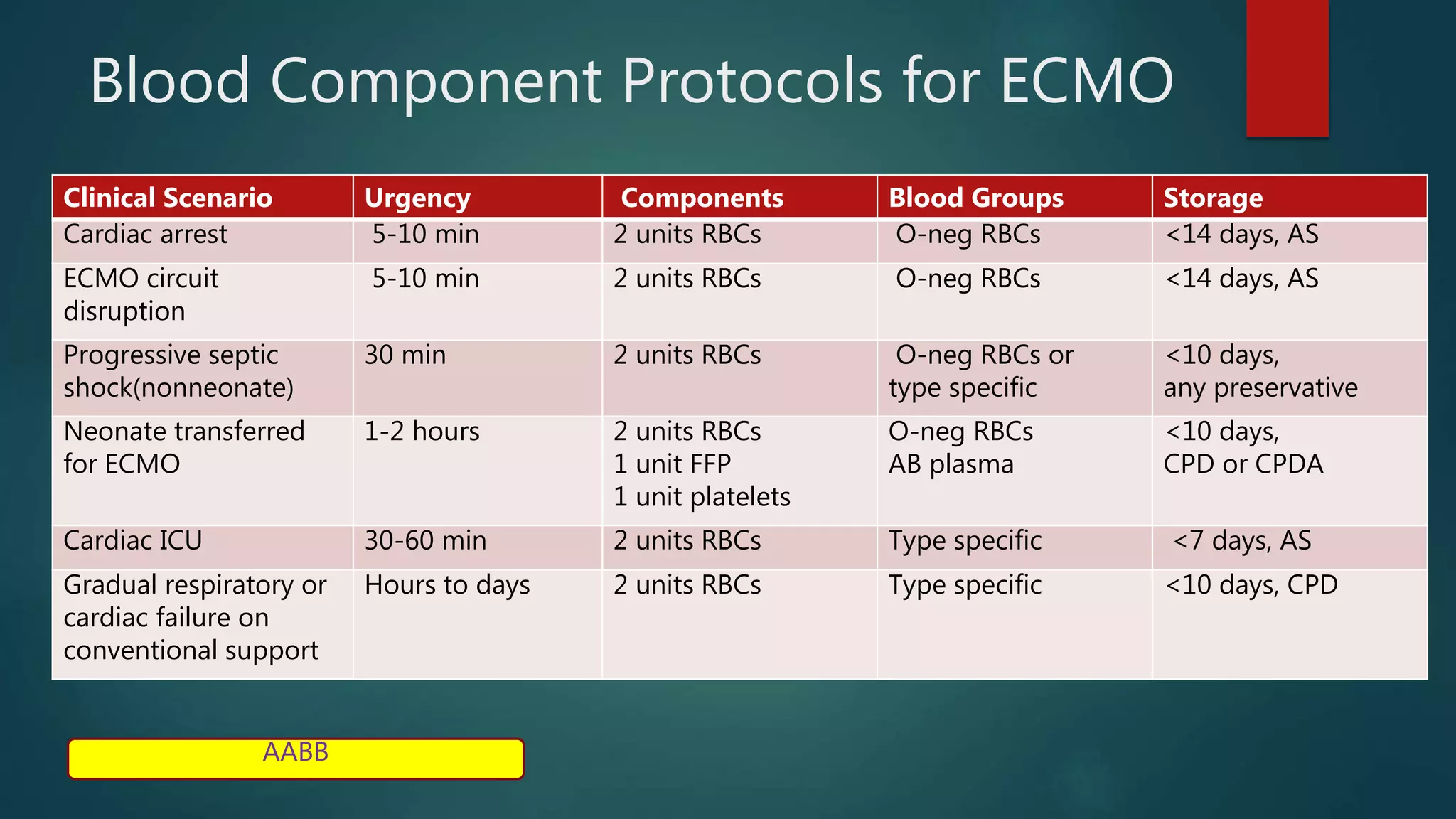





This document discusses extracorporeal membrane oxygenation (ECMO) in adults. It describes the different types of ECMO (veno-arterial, veno-venous, arterio-venous), how the ECMO circuit works to facilitate gas exchange outside the body, clinical indications for its use including acute respiratory failure and cardiac support, complications, and transfusion guidelines for ECMO patients.