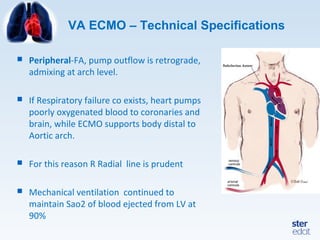
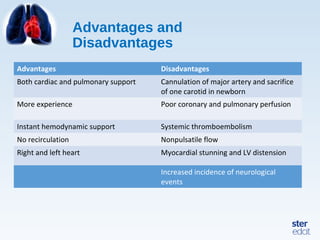
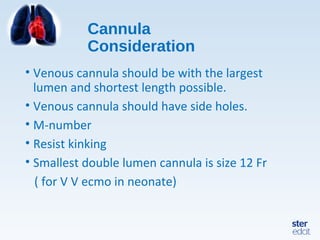
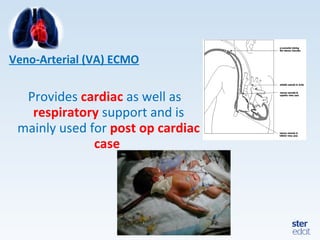
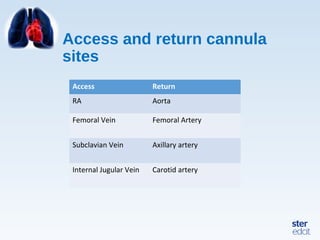
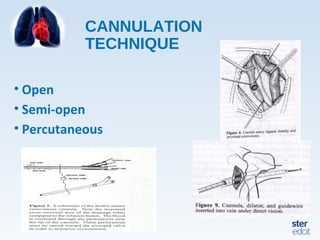
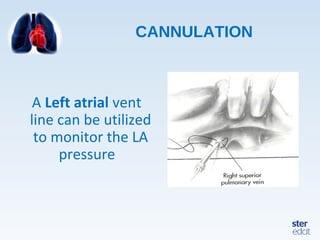
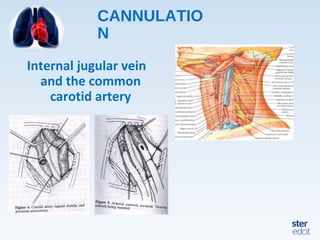
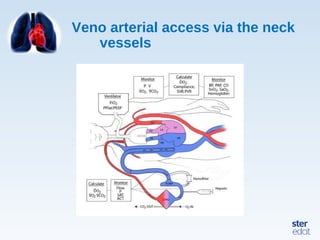
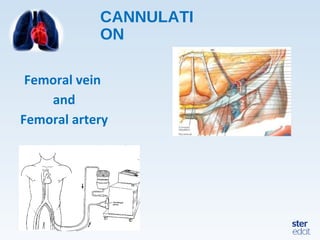
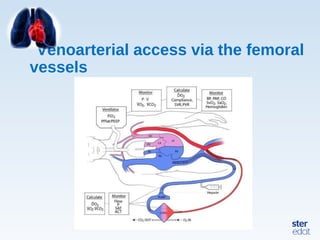
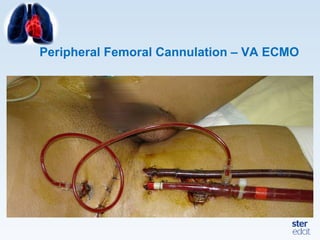
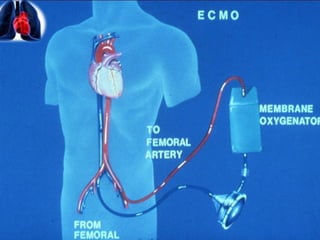
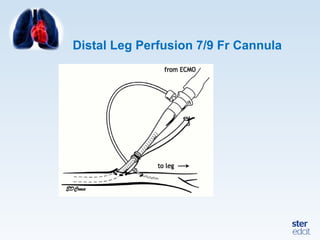
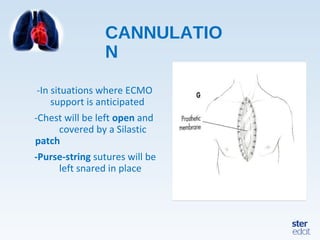
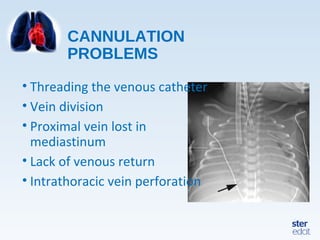
Veno-arterial extracorporeal membrane oxygenation (VA ECMO) provides both respiratory and circulatory support for patients with heart and lung failure. It works by draining venous blood, oxygenating it, and returning it to the arterial system. The document discusses cannulation techniques and considerations for VA ECMO, as well as physiological effects and important monitoring parameters to optimize patient care and outcomes.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

