Extracorporeal technique
Temporary life support
Potentially reversible cardiac and respiratory
insufficiency
Failing to respond to conventional medical
therapy.
Extracorporeal membrane oxygenation (ECMO)
3.
Adaptation ofconventional cardiopulmonary bypass
techniques used in OR for prolonged support in ICU.
Does not treat the underlying disease process.
Aids in recovery by unloading the cardiopulmonary
system.
Can serve as a bridge to organ transplant.
5.
FATHER OF ECMO
In1975,reports of the
first successful instance
of a newborn infant
sustained using ECMO
under the care of
Dr.Bartlett, who is today
called the
‘Father of ECMO’.
For cardiacsupport
Cannulation from a venous side to an arterial
side.
Central – right atrium to ascending aorta.
Periferal – femoral /internal jugular vein to
femoral /carotid artery.
Cannulation sites differs according to the
anatomy and pathology.
VENO ARTERIAL ECMO
9.
Post cardiotomycardiac failure.
Cardiomyopathies
Viral myocarditis.
Bridge to transplant.
Common indications.
10.
In the ICU:the severity defined by pressor and
inotropic requirement, metabolic acidosis,
decreased urine output for 6 hours.
pH<7.25 with raised lactates .
Early postoperative cardiac failure in the operating
room (unable to come off bypass)
Cardiac arrest from any cause
Septic shock without evidence of coagulopathy or
multiorgan damage.
Elective support through high risk catheter
procedures
when to start Ecmo.....
11.
For lungsupport.
Cannulation – from a large vien to another.
femoral vein and internal jugular vein.
Can use a single double lumen cannula.
Veno - venous ecmo
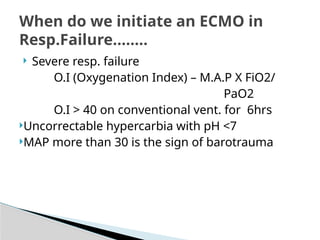
Severe resp.failure
O.I (Oxygenation Index) – M.A.P X FiO2/
PaO2
O.I > 40 on conventional vent. for 6hrs
Uncorrectable hypercarbia with pH <7
MAP more than 30 is the sign of barotrauma
When do we initiate an ECMO in
Resp.Failure........
To treathypercarbia.
No active support to lung.
Ecmo flow through the membrane lung.
Flow is driven by patient’s arterial pressure and
volume load.
It is less invasive and keep the patint in
isobalance state.
ETCO2 REMOVAL