Downloaded 194 times


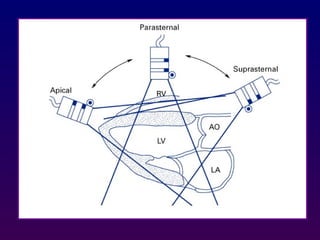
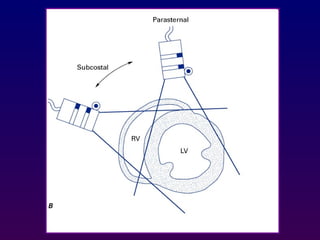
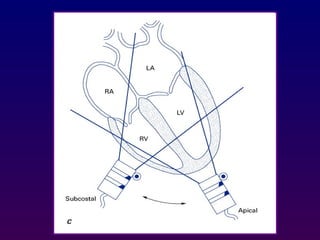
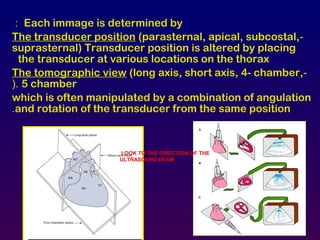
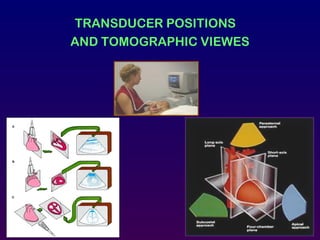
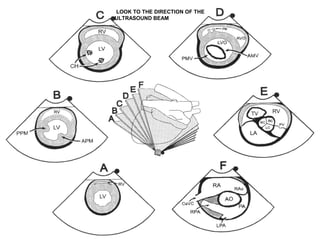
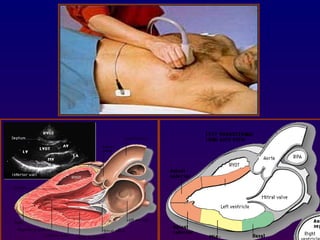
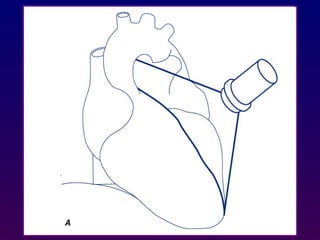
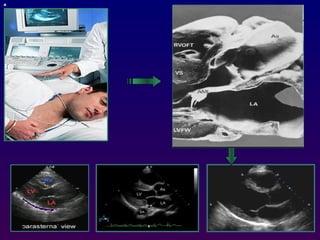
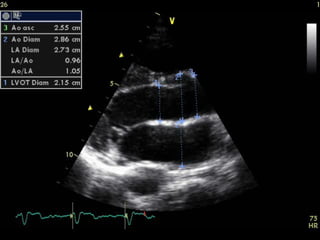
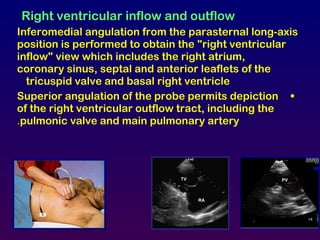
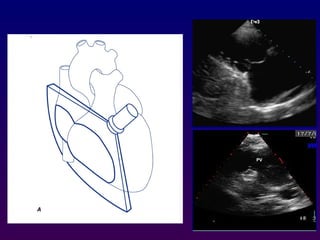


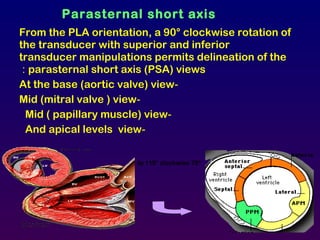
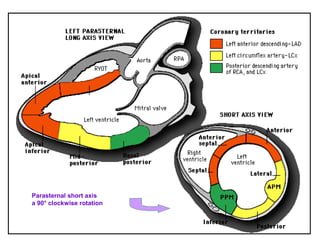
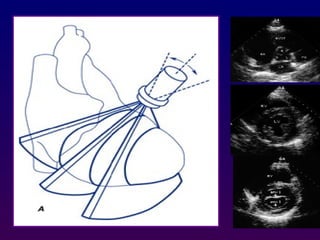
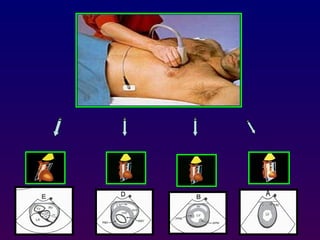

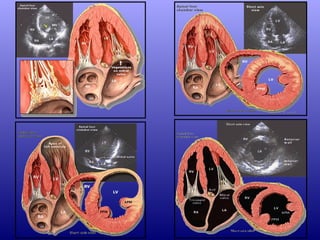
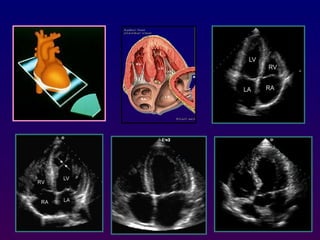
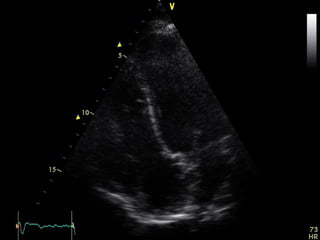
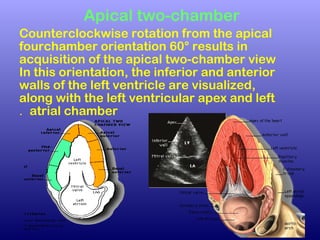
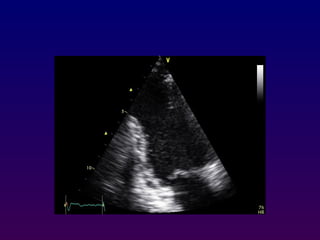
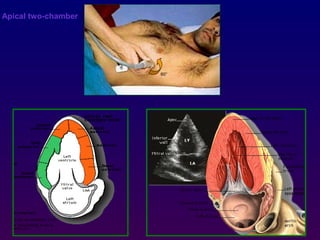

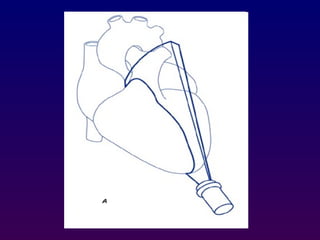
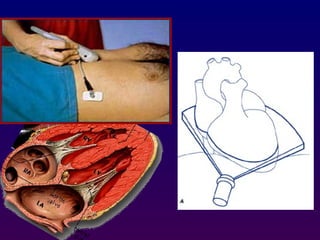
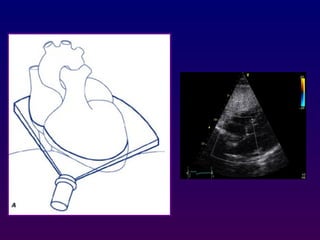

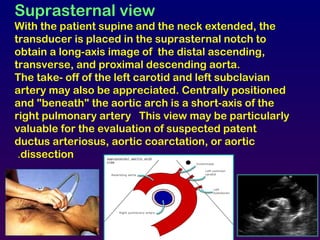
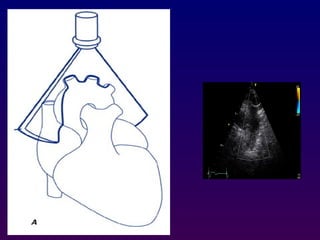
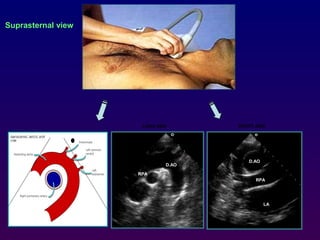

Echocardiography uses ultrasound to examine the heart. Different techniques are used, including M-mode for motion over time, 2D for cross-sectional imaging of anatomy and measurements, and Doppler to study blood flow velocity and direction. Views are obtained by positioning the transducer in different locations and orientations to visualize cardiac structures in various planes, such as parasternal long and short axis, apical 4-chamber, and subcostal. Proper transducer positioning is important for high quality imaging of the heart.









































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

